



Introduction
Benign tumours of the peripheral nerve sheath are uncommon, exact incidence remains unknown and can arise sporadically or associated with genetic disorders. They constitute about 10 – 12% of all benign tumours. They consist of neurofibromas, neurilemmomas or schwannomas, perineuriomas and lipomas etc.1 Schwannomas, formerly called neurilemmomas, are the most common of the benign peripheral nerve tumours; they commonly occur in the head and neck region affecting the cranial nerves, brachial plexus and spinal nerves but less often affects the upper and lower extremities. Involvement of the median nerve has been reported to be about 7 – 14%.2,3 They usually occur between the third to sixth decade of life, with few reports in children.4 Schwannomas are usually solitary tumours but can be multiple in some cases known as schwannomatosis or associated with neurofibromatosis. They are asymptomatic and painless in the early stages, growing slowly over the years preceding diagnosis. They could be symptomatic when they are large as a consequence of compression neuropathy, thereby resulting to pain, paraesthesia, weakness and claw hand in the case of median nerve lesion.2,5 Schwannomas rarely undergo malignant transformation.6
Misdiagnosis is common clinically where it is confused with other benign soft tissue tumour but confirmation is done histologically. Investigative modalities such as electrophysiological study, sonographic study and magnetic resonant imaging can aid diagnosis. There has been some attempt at classification depending on it relation to the nerve fascicles but not widely accepted.1 Treatment is by excision biopsy which may result to nerve injury and deficit in some cases.1,2,5 Children are prone to unintentional injuries which could be due to road traffic accident, domestic and corporal punishments. It has not been reported to result to tumor formation.7
We report a rare presentation of a giant schwannoma of the median nerve in a 13years old child. We also, include the surgical findings, histological reports and functional outcome. This case has not been reported in Western, Eastern and Central African regions.
Case presentation
We present a 13years old girl with 3years history of painless progressively growing solitary tumour on the volar surface of the right forearm. There was associated pain following trauma with cane from her teacher in school where she claim there was a sudden increase in size. No family history of neurofibromatosis. Examination reveal about 7cm mass located on the flexor surface of the forearm close to the wrist, not adherent to overlying but attached to underlying structures. The mass was firm to touch with associated tingling sensation along the distribution of the median nerve and compressive symptoms on the flexor muscles / tendons evident by inability to fully extend the fingers with slight claw hand deformity. There was no wasting of the thenar eminence [Figures 1 & 2]. No swelling on other location on the same limb and any previous surgical scar. We did not do ultrasonographic (USS), nerve conduction (NCS) and magnetic resonance imaging (MRI) studies. The reason we did not do NCS and MRI was due to cost (patient did not have health insurance) but for USS, it was an oversight. However, a plain radiograph of both limbs was done which showed a soft tissue shadow not arising from bone.


We made a working diagnosis of intraneural lipoma to exclude traumatic cyst, based on this she was scheduled for excisional biopsy. A written informed consent was given by the mother to proceed with the operation and for publication of images with preservation of privacy.
A longitudinal incision was made on the volar surface of the right forearm centred on the tumour with patient under Biers block. Incision was deepened with meticulous dissection exposing the tumour and demonstrating its intraneural location with nerve fascicles overlying it [Figure 3]. This corresponds to a type 3 tumour.1 The tumour was enucleated by a longitudinal incision between nerve fascicle visible to the ordinary eyes [Figures 4 & 5]. The nerve sheath was repaired and dead space obliterated and wound closed without repairing subcutaneous fascia.



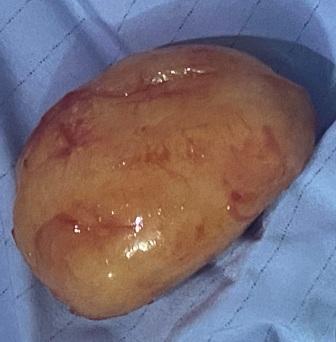
The tumour removed was an oval shaped, yellow and encapsulated. The cut surface showed areas of central necrosis. Histopathological report showed two main patterns, hypercellular Antoni A cells and myxoid hypercellular Antoni B cells. We could not provide the slides due to delay in obtaining the results (financial constraint) during which it was discarded.
The patient recuperated with no nerve deficit. There was improvement in hand movement and function. Subsequent follow up reveals no new symptom by the patient and she has fully integrated into society.
Discussion
Schwannomas of the median nerve is the most common of the benign peripheral nerve sheath tumour. Most of the cases reported in literature were found in adults2,3,5 but very little report in children.4 Our index case was a child.
Some authors have reported nerve deficit pre-surgery in their patients with giant schwannomas which resolved post-surgery. In the index case, there was no obvious nerve deficit but compressive symptoms [Figure 2].2,5
The diagnostic dilemma associated with clinical diagnosis of the tumour was encountered by our team; this was resolved by characterization of the tumour histologically.2,3,5 The tumour excised when grossly examined was found to have an area of degeneration which is due to inadequate blood supply. An author described it as ancient schwannoma.2
According to Holzbauer et al1 the index tumour was a type 3 in terms of the relationship of the tumour to the nerve fascicles.
Despite numerous reports of the tumour, there has been no documented recurrence with complete enucleation of the tumour.8
The index case presented has a history of trauma which was a red herring necessitating our initial diagnosis of traumatic cyst and lipoma. Schwannomas has been associated with misdiagnosis as reported in some literatures.2,5
No author has reported any sex or race predilection, our index case was a girl.2–5
The strength of this case report is that, it has never been reported in Western, Eastern and Central African region. The inability to provide the histological slides was a limitation.
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conclusions
Schwannomas of the median nerve is a rare tumour that has not been frequently reported to affect children. High index of suspicion with tissue histological characterization is needed to confirm the diagnosis. Surgical enucleation is the mainstay of treatment with the preservation of nerve function.