INTRODUCTION
Globally, road traffic accidents (RTA) are on the rise with motorcycle users being among the most vulnerable groups. They are prone to encountering high morbidity and mortality. According to World Health Organization (WHO), approximately 1.3 million people globally die each year due to road traffic crashes, with 20 to 50 million more people sustaining non-fatal injuries leaving them with significant disabilities.1 Approximately 93% of the world’s fatalities on the roads happen in low and middle-income countries (LMICs) even though roughly 60% of the world’s vehicles dwell in these settings. It is estimated that more than half of all road traffic deaths are among vulnerable users including motorcyclists.1
The burden of Road Traffic Injuries (RTIs) is on the rise, causing significant economic losses to individuals, their families, and nations. Even in developed countries, people from lower socioeconomic backgrounds are more likely to be involved in road traffic accidents. The economic burdens resulting from these accidents are multifaceted, stemming from treatment costs, loss of productivity and valuable working time for victims and relatives, loss of skilled labor force, and loss of school hours. Road traffic accidents impose substantial economic costs, with most countries losing approximately 3% of their Gross Domestic Product (GDP) annually.1 Furthermore, RTIs have become the leading cause of death among people aged 5-29 years, disproportionately affecting vulnerable groups such as pedestrians, cyclists, and motorcyclists, particularly those living in developing countries.1,2
It is estimated that approximately 770 million motorcycles are on the roads worldwide, engaging in various activities.3 In developing nations, motorcycles are utilized for essential responsibilities related to transportation and economic activities. Motorcycle accidents account for more than 380,000 annual deaths globally, with 28% of fatalities occurring in 2016, primarily in the African region.2,3 Sub-Saharan Africa, in particular, faces a rapidly increasing burden of trauma from road accidents, which has been termed “Africa’s silent epidemic”.4
In developing countries, motorcycle injuries have become a pressing yet overlooked public health concern, substantially contributing to road traffic accidents and fatalities.5,6 In spite of the increased risks which is reported to be 30 times more likely to be fatal and eight times more likely to result in injury compared to other vehicles, motorcycles are increasingly popular due to their convenience.7 Commercial motorcycling has become widespread in rural and urban areas, leading to significant morbidity and mortality, particularly in sub-Saharan Africa, where young people rely on motorcycles for transportation and livelihood, driven by high unemployment rates.5
Malawi is experiencing rapid economic growth and a surge in motor vehicle registrations, including motorcycles. The country’s estimated road traffic fatality rate stands at 35 deaths per 100,000 people per year, the second-highest globally.8,9 In Malawi, as in other developing countries, motorcycle road traffic accidents are rising due to increased motorcycle taxi operations. Most motorcyclists operate illegally, lacking driver’s licenses and helmets, putting themselves and vulnerable road users at greater risk. Their limited knowledge of road traffic rules exacerbates this risk. Consequently, crash victims often present to hospitals with various injuries, frequently including orthopedic trauma. Despite the growing number of trauma patients and substandard care leading to poor outcomes, research remains scarce. This study aimed to investigate patterns of orthopedic injuries, demographic characteristics, and injury mechanisms among motorcycle trauma patients admitted to Queen Elizabeth Central Hospital.
METHODS AND MATERIAL
A retrospective study was conducted at Queen Elizabeth Central Hospital (QECH), the largest referral and teaching hospital in Blantyre, southern Malawi. QECH primarily serves the southern region, comprising 13 districts with a population of approximately 7.75 million.10 Due to the lack of a district hospital in Blantyre, QECH also provides primary and secondary services. The hospital has a bed capacity of 1,200.
Data on road traffic accident (RTA) patients from January to December 2021 were retrieved from an electronically maintained orthopedic database. This information facilitated the location and identification of patients’ files from the hospital’s Health Management Information System (HMIS) office. All available patient files admitted to orthopedic wards due to RTA were collected, and the total number was recorded. From this total, only files of patients involved in motorcycle accidents were selected and stored using Research Electronic Data Capture (REDCap).
The following data were collected: demographics (age, gender, education status, occupation, and place of residence); accident details (accident scene, mechanism of injury, patient’s role, and helmet use); clinical information (presenting features, associated injuries, treatments, and duration of hospital stay); and treatment outcome (discharged or deceased). Injury patterns were noted by reviewing documented diagnoses based on clinical and radiographic assessments.
Descriptive statistics were used to summarize the data, with categorical variables presented as frequencies and percentages, and continuous variables described using means and standard deviations.
For inferential statistics, the chi-square test was employed to examine the association between dependent and independent variables. Additionally, binary logistic regression analysis was conducted to determine the magnitude and direction of association, yielding crude and adjusted odds ratios. All inferential statistical tests were performed at a 95% confidence level using SPSS version 27. A p-value < 0.05 was considered statistically significant.
This study received approval from both the Hospital Research Committee and College of Medicine Research and Ethics Committee (COMREC).
RESULTS
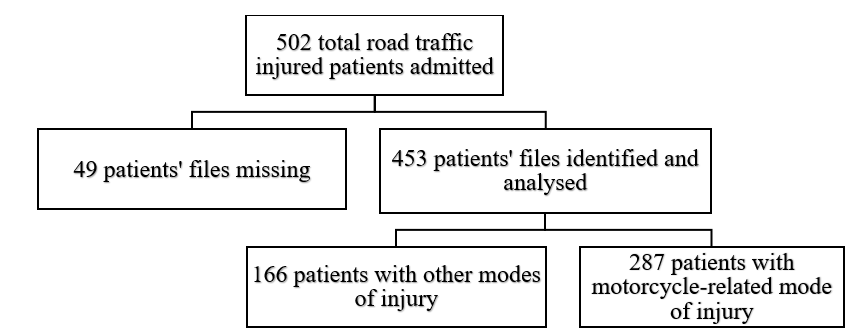
A total of 502 road traffic trauma patients were recorded in the inpatient orthopedic trauma database. Of these, 453 patients’ files were identified and analyzed, while 49 files, representing 9.7% (49/502), were missing and hence not analyzed. Among the 453 analyzed patient files, 287 patients, representing 63.4%, (287/453), suffered motorcycle injuries, accounting for the majority of road traffic accidents (Fig. 1).

Demographic Features of the Groups Commonly Involved in Motorcycle Accidents.
Gender
Most of the victims in this study were male, 78.7% (226/287) whereas 21.3% (61/287) were female.
Age
The age range of patients was 8 to 78 years, with the majority falling within the productive age group of 21 to 40 years, 53.7% (154/287). The mean age was 34.4 (SD 13.8).
Education
Data on education status was unavailable for 69.3% (199/287) of patients. Among the remaining patients with available data, 40.9% (36/88) had attended primary education as their highest level of education, 27.2% (24/88) of patients had attended secondary education, 20.4% (18/88) of patients had attended tertiary education. Notably, 11.4% (10/88) of patients did not attend any formal education.
Occupation
Occupation status data was available for only 38.3% (110/287) of patients. Among these, the majority were businesspeople, including motorbike taxi operators, accounting for 45.5% (50/110) of the sample. Workers/employees comprised 22.7% (25/110) of the patients, followed by farmers at 19.1% (21/110) and students at 12.7% (14/110).
Area of Occurrence of Motorbike Accidents
There was missing data in 7.3% (21/287) of the study population about the area of occurrence of motorbike accidents. However, among those with available data, urban areas had a higher incidence rate of motorcycle accidents, 64.1% (168/266), compared to rural areas, 35.9% (94/266). The highest rate was observed in Blantyre urban, 56.7% (151/266), and very few in Blantyre rural, 6.8% (18/266). The referral cases from areas outside Blantyre accounted for 36.5% (97/266).
Role of the patient
Data on the patient’s role at the time of the accident was available for 96.2% (276/287) of the study population. The majority of victims were motorcycle drivers, 42.8%, (118/276), followed by passengers, 36.2% (100/276) and pedestrians 21.0% (58/276).
Relationship between Socio-demographic Characteristics and Motorcycle Accidents Involvement
A chi-square test at a 95% confidence level examined the association between patients’ demographic characteristics and their involvement in motorbike accidents. For this analysis, involvement was categorized as active (drivers/passengers, referred to as motorbike users) or passive (pedestrians, referred to as non-motorbike users).
The results, presented in Table 2, reveal significant associations between active involvement in accidents and three demographic factors: age (p = 0.001), accident site (p = 0.014), and area of residence (p = 0.013). Conversely, no significant relationships were found between active involvement and gender (p = 0.38), occupation (p = 0.371), or education (p = 0.179).
Based on logistic regression analysis, patients aged 21-40 were 3.15 times more likely to be actively involved in motorbike accidents compared to those aged 0-20 (AOR 3.15, 95% CI: 1.433-6.939). Similarly, patients aged 41-60 had a 3.5-fold increased likelihood (AOR 3.5, 95% CI: 1.332-9.185). Conversely, patients over 60 were 65% less likely to be involved (AOR 0.349, 95% CI: 0.09-1.36).
Patients with urban accident locations were 1.35 times more likely to be actively involved in motorbike accidents than those with rural locations (AOR 1.348, 95% CI: 0.323-5.617). In Blantyre, urban residents had a 1.36-fold increased likelihood of active involvement compared to rural residents (AOR 1.364, 95% CI: 0.317-5.863). Notably, residents outside Blantyre district (referral areas) were 3.54 times more likely to be actively involved than Blantyre rural residents (AOR 3.54, 95% CI: 0.939-13.35).
Mechanism of Injuries among Motorcycle Trauma Patients
Only one victim (0.3%, 1/287) lacked data on motorcycle injury mechanism. Among those with data, collisions between motorcycles and cars were the most common injury mechanism, accounting for 41.6% (119/286) of cases (Table 3).
Outcome on Discharge
Three patients (3/287) lacked discharge outcome documentation, resulting in 1% missing data. Among those with data, the majority were discharged home, 97.5% (277/284), while 2.5% (7/284) died during treatment. Notably, 85.7% (6/7) of deceased patients had concomitant non-orthopedic injuries, and 71.4% (5/7) succumbed within 7 days of orthopedic admission.
Relationship between Demographic Characteristics, Injury Mechanism, Length of Hospital Stay and Survival (Treatment Outcome)
A chi-square test analyzed the relationship between gender, age, injury mechanism, length of stay, and discharge outcome. The results, presented in Table 4, showed significant associations between discharge outcome and two variables: injury mechanism (p = 0.017) and length of stay (p = 0.001). In contrast, no significant relationships were found between discharge outcome and gender (p = 0.621) or age (p = 0.500).
Logistic regression analysis revealed that patients involved in motorbike-car collisions were 14.76 times more likely to die compared to those with non-motorbike car collisions (AOR 14.76, 95% CI 1.619-34.65). Non-motorbike car collisions included falls from motorbikes after losing control, motorbike-motorbike collisions, and pedestrians hit by motorbikes.
Regarding hospital stay duration, patients staying over a week were 95.8% less likely to die compared to those staying less than a week (AOR 0.042, 95% CI 0.007-0.242). This indicates that deceased patients were more likely to die within the first week of admission.
Patterns of Orthopedic Injuries in Motorcycle Accidents.
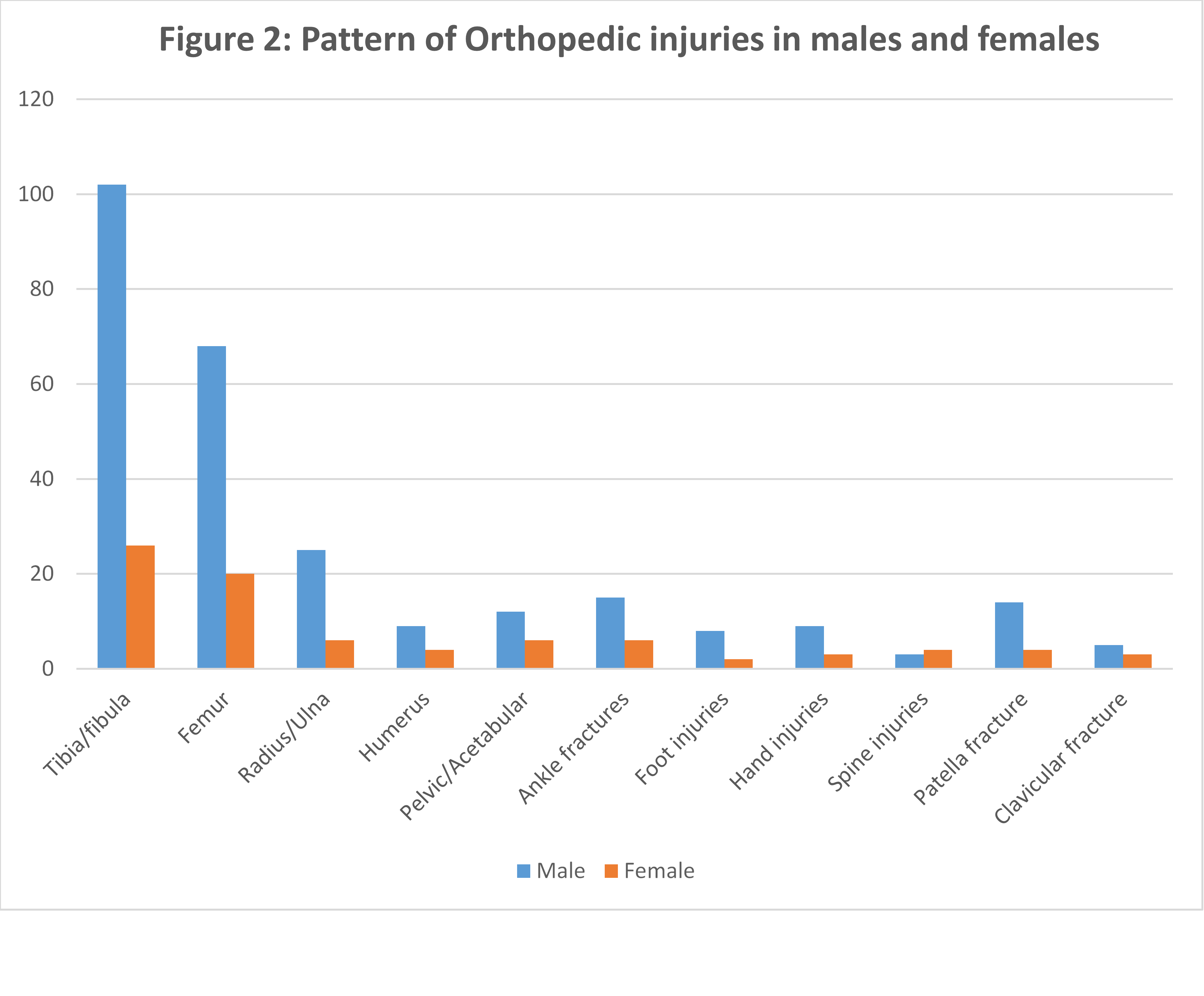
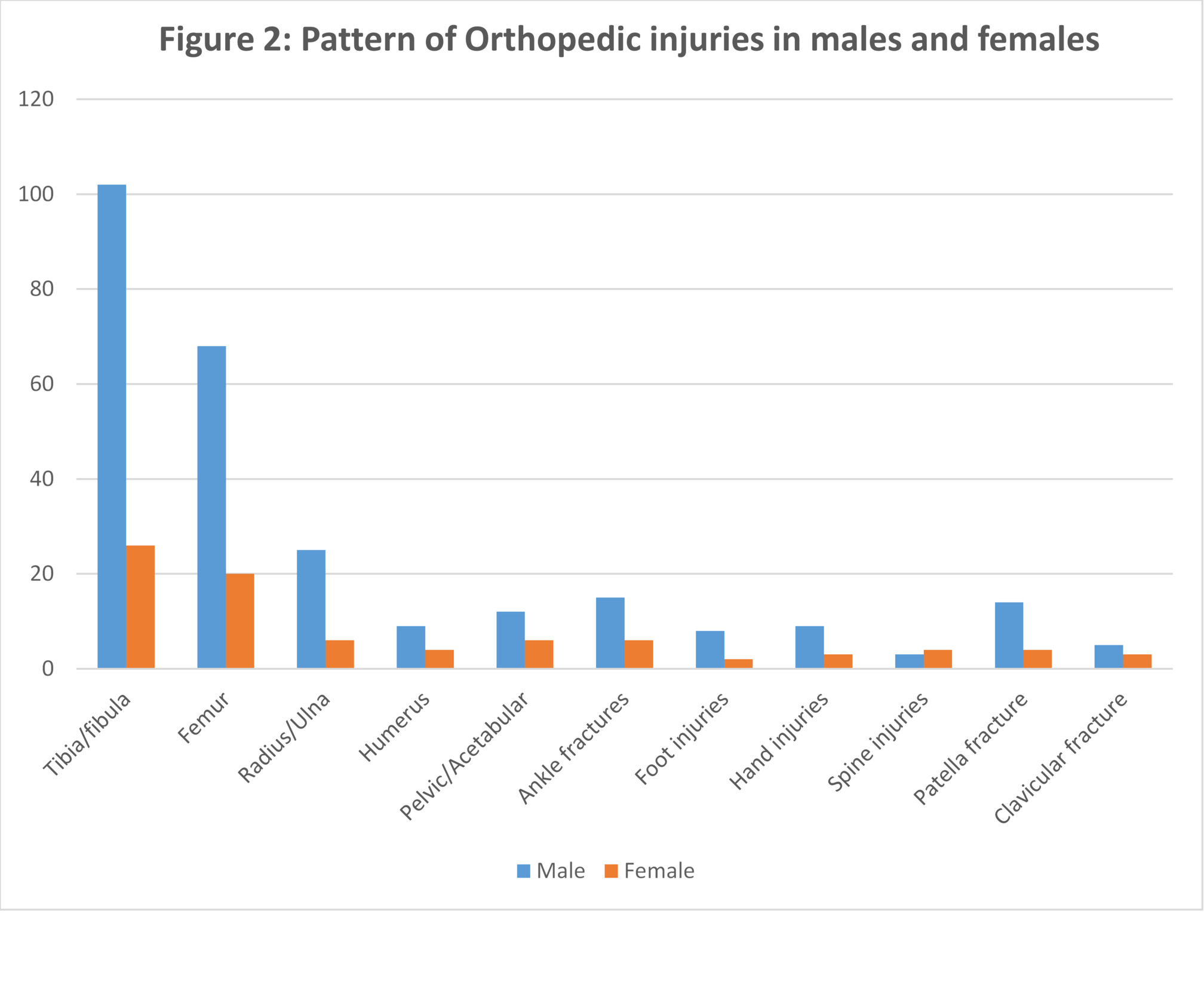
The most frequent orthopedic injury pattern was lower limb fractures, with the tibia and fibula being the most common among the patients, 44.6% (128/287), followed by femur fractures 30.7% (88/287) (Table 5).
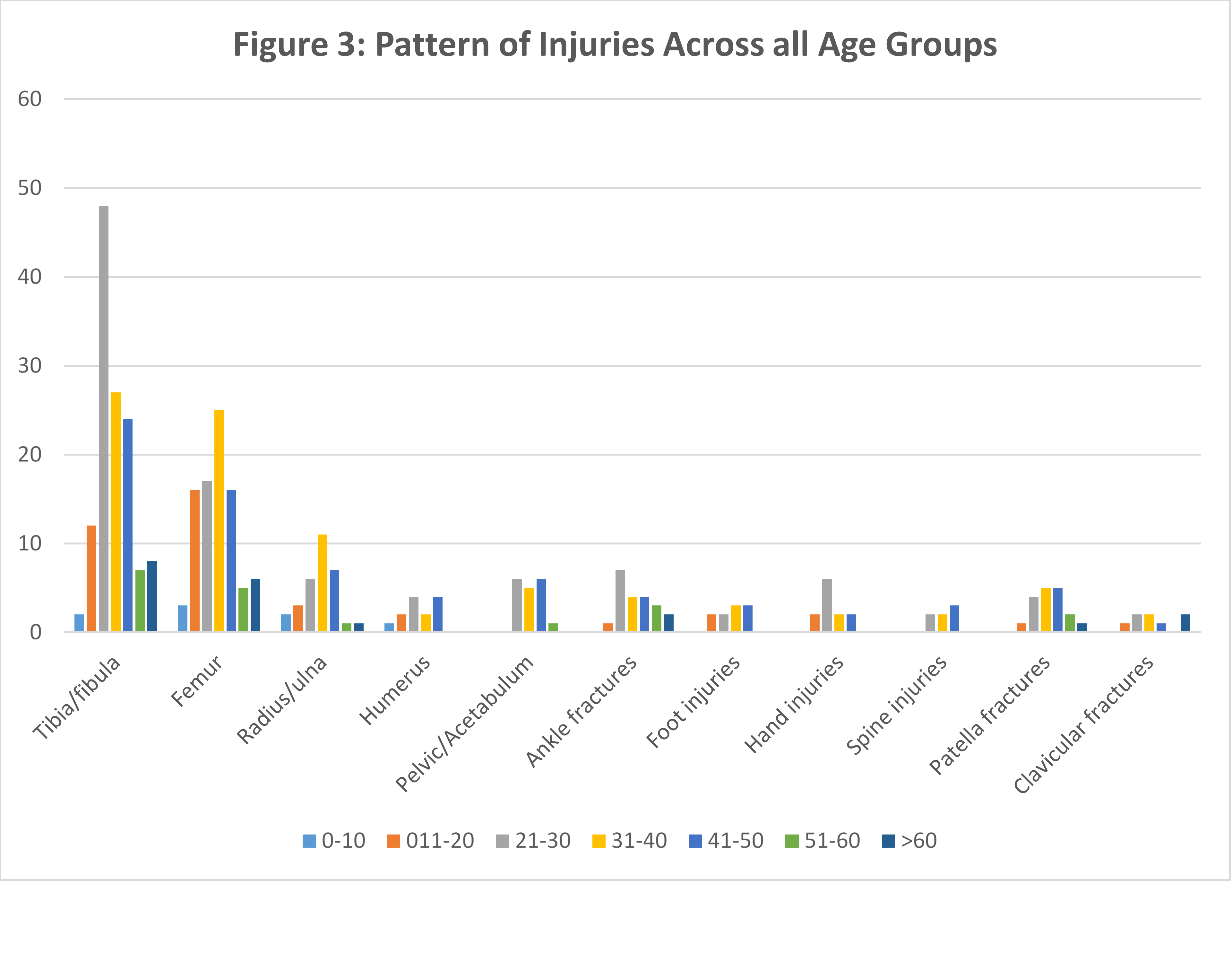
A similar trend in injury patterns was observed across both genders, with tibia and fibula fractures being the most common (Fig. 2). Similarly, tibia and fibula fractures predominated across age groups, except among those under 20, where femur fractures were most prevalent (Fig. 3).

Relationship between Gender, Age, Mechanism of Injury and Injury Pattern
A chi-square test of association was conducted to examine the relationship between gender, age, mechanism of injury, and patterns of injury. Injury patterns were categorized into lower limb fractures and upper limb fractures. Mechanisms of injury were classified into two groups: vehicle collisions (e.g., motorbike-motorbike, motorbike-car collisions) and non-vehicle collisions (e.g., falls from motorbikes after losing control, being hit by a motorbike). The results showed no statistically significant association between any of the variables and injury patterns (p > 0.05).
Fracture Patterns: Open vs. Closed
Closed fractures comprised 64.5% (185/287) of all fractures, while open fractures accounted for 35.5% (102/287). Among the open fractures (n=102), tibia/fibula fractures represented 57.8% (59/102). A chi-square test of association between fracture location and openness revealed a significant correlation between tibia/fibula fractures and increased likelihood of being open (p=0.001). Notably, 46.1% (59/128) of tibia/fibula fractures were open.
Based on the logistic regression analysis, patients with tibia/fibula fractures were 2.31 times more likely to have an open fracture compared to those with other fractures combined (odds ratio: 2.307; 95% CI: 1.409-3.777).
Orthopedic Injury Patterns and Treatment
In terms of treatment provided, data was lacking for 1% (3/287) of the total study population. For those with available data, the majority of orthopedic injuries underwent surgical treatment (70.1%, 199/284), while 29.9% (85/284) received non-surgical/conservative treatment. The most common duration of hospital stay ranged from 1 week to 1 month, with the majority (43.9%, 125/285) being discharged within 14 days (Table 1).
Associated Non-Orthopedic Injuries
Among orthopedic ward admissions, 16.7% (48/287) sustained concurrent non-orthopedic injuries. Head injuries were the most common associated non-orthopedic injuries, accounting for 81.3% (39/48), followed by blunt abdominal trauma at 10.4% (5/48) and chest injuries at 8.3% (4/48).
DISCUSSION
Motorcycle usage in Malawi, mirroring trends in other developing countries, is experiencing exponential growth as a primary transportation mode.8 However, this increase is accompanied by a concerning rise in road traffic accidents. Our study revealed that nearly two-thirds (63.4%) of trauma orthopedic admissions resulted from motorcycle accidents, aligning with Banza et al.'s study (2018) which reported that vulnerable road users, including motorcyclists and pedestrians, accounted for nearly two-thirds of road traffic injuries.8 The widespread disregard for traffic rules and regulations among motorcycle riders, coupled with the lack of licensure among the majority on public roads, plays a significant role. Additionally, the inherent vulnerability of motorbikes due to their lack of protective features compared to enclosed vehicles further elevates the risk. Consequently, these factors increase the likelihood of accidents and injuries among motorcyclists and other vulnerable road users.11,12
Most motorcycle accidents occurred in urban Blantyre, contrasting with rural areas of Blantyre and surrounding districts. This disparity may be attributed to the higher motorcycle usage in urban areas, driven by increased business activity and commuting. Furthermore, elevated road traffic in urban areas increases the likelihood of collisions with other vehicles. However, potential biases in case reporting may also contribute to this disparity. Specifically, some orthopedic trauma patients from district accidents may not be referred to our facility, while severely injured patients from distant areas may succumb to injuries before arrival. Notably, Blantyre’s lack of a district hospital funnels patients directly to our facility, potentially increasing Blantyre urban accident numbers.
The majority of patients involved in motorbike accidents were businesspeople, including motorbike taxi operators. This finding is consistent with previous studies highlighting the increased risk of road traffic injuries among commercial motorcyclists.11 The high representation of motorbike taxi operators in our findings may be attributed to their increased exposure to road traffic, prolonged working hours, and potentially hazardous driving practices. Additionally, workers/employees, farmers, and students were also commonly involved in motorbike accidents.
This study revealed that 78% of motorcycle injury victims were males in their reproductive years, likely attributable to socioeconomic factors. Men are more likely to use motorcycles as employment or transport to their job. It is not uncommon to see men driving motorcycles and engaging in taxi services, whereas women are predominantly passengers or pedestrians, often victims of these accidents. Notably, no female victims in this study were the drivers at the time of accidents reflecting societal norms influenced by cultural backgrounds. Young men frequently engage in leisure driving, increasing their likelihood of drinking and driving, speeding, and other risky behaviors. Consistent with prior research, males in their productive years exhibit high motorcycle accident rates due to reckless riding practices, including helmet avoidance, overloading, speeding, and substance-impaired driving.11–13
A significant proportion of motorcycle accident victims had a low educational background, with a substantial majority having only completed primary education as their highest level of educational attainment. This finding is consistent with existing research, which has consistently demonstrated that individuals with elementary education are disproportionately represented in motorcycle road accidents, and are more likely to experience high case fatalities.14,15 Individuals with little or no education are likely to come from low socioeconomic background and therefore are inclined to choosing the cheapest mode of transportation including motorcycles. They are also likely to engage in motorbike taxi operations as their business to generate income to support their families. Generally, less educated people are less likely to drive cautiously, less aware of traffic rules and regulations and therefore prone to fatal accidents.
In this study, collisions between motorcycles and other vehicles were found to be the most common mechanism of injury, consistent with observations in similar studies.11,16–18 Motorcycle drivers themselves were the most frequent victims of accidents, followed by passengers. As most motorcycle riding occurs in urban settings, where other vehicles are numerous, the likelihood of motorcycles colliding with cars is high, particularly when navigating through traffic congestion. In developing countries, poor road conditions, overspeeding, and overloading of vehicles and motorcycles with passengers or luggage increase the risk of collisions between motorcycles, other vehicles and pedestrians. This situation is exacerbated by a lack of understanding and/or adherence to road traffic signs and signals among many road users.
Several studies have demonstrated that motorcycle trauma victims present to hospital with different pattern of injuries including neurosurgery, general surgery and orthopedic surgery trauma conditions but orthopedic injuries are commonly encountered.5,12 The most common pattern of orthopedic injuries in this study was that of lower limbs with fractures of tibia/fibula being the commonest followed by femur fractures. Our findings are consistent with similar studies done elsewhere which demonstrated similar pattern, with the fractures of tibia/fibula being the commonest.7,11,12,19 Due to anatomical position and superficial subcutaneous location of the tibia/fibula, they are prone to fracture and are highly susceptible to becoming open fractures during road traffic accidents.20,21 Notably, our study found that 46.1% of all tibia fractures were open. However, of all the fractures together, 35.5% were open with tibia/fibula fractures accounting for 57.8% of these open fractures.
The global burden of orthopedic injuries is substantial, exerting significant pressure on healthcare resources, including in low-resource settings like Malawi. The consequences of these injuries are devastating, affecting not only the individual but also their families and communities. Prolonged hospitalizations result in increased healthcare utilization, reduced productivity, and long-term disability.11 Our study’s findings indicate that hospital stays for orthopedic injuries ranged from less than 7 to more than 30 days, with a median duration of 14 days. Injury severity, pattern, and treatment modality significantly influenced hospitalization duration. Notably, surgical intervention was the primary treatment approach, yielding shorter hospital stays compared to conservative management with skeletal or skin traction. This is consistent with existing literature, which highlights the impact of multiple injuries and comorbidities on prolonged hospitalization.11
This study found a 2.5% mortality rate among orthopedic ward admissions, contrasting with similar studies done in Egypt (1.9%) and Pakistan (1.1%).11,12 The higher mortality rate in our study may be attributed to concomitant life-threatening non-orthopedic injuries, potentially overlooked or missed during admission. Our study found that those that died, 85.7% had concomitant non-orthopedic injuries and head injury was the commonest. Other study findings have revealed head injury as the leading cause of death in trauma patients.12,22 Most deaths (72.7%) occurred within 7 days of admission, but specific causes of death were not recorded in our study.
Notably, when considering all motorbike trauma patients, regardless of whether they sustained orthopedic and/or other injuries, the mortality rate exceeds the rate observed in our study.12,13,17 Our findings indicate that collision between motorcycle and a car was significantly associated with increased mortality, likely attributable to the high-energy impact and resultant multiple injuries.
The study’s reliance on patient file data introduces potential biases and limitations characteristic of retrospective research. Specifically, missing and incomplete data were encountered in some variables under investigation. Another limitation stems from the potential bias introduced by missing patient’s files and the exclusion of multisystem injured patients admitted to wards outside the orthopedic department. Furthermore, this single-centered study creates a selection bias that potentially would affect external validity.
These limitations may impact the generalizability and representativeness of the findings. To address these concerns, future studies should consider several key improvements. Specifically, adopting multicenter designs would enhance external validity, while comprehensive data collection strategies would minimize missing values. Additionally, employing inclusive criteria would capture diverse patient populations, and implementing strategies to mitigate selection bias would strengthen the reliability of the results. Furthermore, conducting prospective studies would provide more accurate and reliable data.
Despite the limitations, this study contributes significantly to our understanding of the epidemiological characteristics surrounding motorcycle accidents. The findings have important implications for prevention strategies, policy development, and healthcare resource allocation focused on mitigating the impact of motorcycle accidents. Future research can enhance these results by employing more superior study designs, ultimately yielding higher-quality evidence to inform motorcycle safety initiatives.
CONCLUSION AND RECOMMENDATIONS
Motorcycle accidents are a frequent cause of road traffic accidents and pose a significant public health challenge in Malawi. These accidents lead to a high burden of morbidity and mortality, primarily affecting the productive age group, young men in particular, leading to socioeconomic downfall on individual family and the country at large.
We recommend that policymakers should consider preventive measures, as the treatment of these injuries strains already limited hospital resources and contributes to poor patient outcomes. Such preventive measures include educational campaigns through various media, enforcement of traffic rules and regulations including making sure the motorcycle drivers undergo an appropriate training before licensure. We also recommend that the responsible authority should restrict operation of motorcycle taxi (locally called kabaza) in busier public roads, for example, in city urbans where most of the motorcycle accidents occur as shown in this study. In addition, improving safety of road infrastructure through introduction of pavements and special road crossing for pedestrians in busier public roads are other important safety measures.
ACKNOWLEDGEMENTS
This project is an output from the Global Surgery Research Programme, funded by the Irish Aid for the RCSI/COSECSA Collaboration Programme.
Special acknowledgment goes to the following individuals for their roles to bring this research project to success:
Ms. Jennifer Msowoya, for the role of data collection and entry into Research Electronic Data Capture (REDCap).
Mr Wongani Mtabayira Nyondo, for the role of data analysis and interpretation.