Introduction
Access to quality healthcare remains a critical issue in developing low- and middle-income countries, where resources are limited, and there is limited data on healthcare standards and quality of care. A literature review reveals that studies on the standards of care, particularly in Sudan, are limited. One notable study has highlighted the importance of academic partnerships in enhancing the quality of pediatric surgical care in Sudan, highlighting the need for further exploration in other surgical fields.1
Since a 1993 consensus conference established LC as the preferred treatment for gallstone disease, LC has become the standard of care globally due to its minimally invasive nature and reduced recovery time.2 However, in LMICs, limited access to advanced laparoscopic equipment and the high cost of such procedures make LC less accessible. MC is a suitable alternative to LC, particularly in complex cases, such as acute cholecystitis, empyema, or gallbladder mucocele. The operation is defined as a procedure for removing the gallbladder using a 3-6 cm incision in the right upper quadrant performed in the standard open surgical setting. This procedure is associated with fewer complications and a shorter postoperative recovery period in comparison to regular open cholecystectomy, making it suitable for settings with limited resources3,4
The high cost of minimally invasive surgery in LMICs highlights the need for cost-effective, practical, and safe approaches that can be adapted to resource constraints. MC offers a feasible alternative in such settings by providing safe and effective outcomes with lower resource demands, as shown in some studies.4–7 The objectives of this study were to determine if MC can serve as both an effective and safe treatment for gallstone disease and a sustainable training standard adapted to the practical realities of the limited resources in Eastern Sudan.
Patients and Methods
This single-blinded, prospective descriptive, and analytical study was conducted in surgical health facilities in Kassala State, Sudan, from January 2018 to December 2021. All patients presenting with gallstone disease who underwent mini-cholecystectomy during this period were included, with no exclusion criteria. This approach allowed for a comprehensive, convenient sample of all eligible patients within the specified timeframe. Written informed consent was obtained from each patient or their legal guardian before the procedure, and all methods adhered to relevant regulations and guidelines. The Ethics and Research Committee of Kassala Police Hospital granted ethical approval. A control group of two consultants was compared to an index group of eight trainee registrars who had completed specific training in mini-laparotomy cholecystectomy and could perform the procedure independently. Data were collected prospectively from patient records, directly observing patient outcomes over a one-year follow-up period. Variables included operator role (consultant or registrar), patient demographics (age, gender, and comorbidities), diagnosis, hospital stay duration, biliary injury incidence, postoperative vomiting, and pain management (analgesia and opioid use). Pain management protocols were standardized across both groups to ensure uniformity in postoperative care, and a Visual Analog Pain Scale was used to assess pain severity. Discharge Criteria were stable vital signs, pain control, oral intake, absence of complications, mobilization, normal urinary function, and understanding of postoperative care. To calculate the sample size, the significance level was set at 0.05 (5%), and power was set at 80% to detect a true difference. An appropriate formula was used using prior data. After calculations and adjustments, the total was set at 600 patients, allowing sufficient statistical power to detect differences in the key outcomes across the two groups. All patients admitted within the study period were included to avoid selection bias. The relevant guidelines and regulations followed the rules and principles of the Helsinki Declaration of 1964 for medical research. All patients consented to participate in the study and publication of the results. All patient’s data were analyzed anonymously to ensure confidentiality.
Operative Procedure
The procedure commenced with confirmation of diagnosis and acquisition of informed consent. Patients were positioned supine on a bridging table, and general anesthesia was administered. The skin was prepped and draped for the aseptic technique. A right subcostal transverse incision was made through the abdominal wall down to the peritoneum. Deaver’s retractor and bowel gauze were used for retraction, with traction applied to the gallbladder fundus. Dissection of Calot’s triangle was performed, followed by ligation and division of both the cystic artery and cystic duct. The gallbladder bed was then dissected from the liver, and closure was achieved in layers.
Data Analysis
Data were analyzed using SPSS version 21.0, with statistical significance set at P < 0.05 and a 95% confidence interval. Frequency distributions of variables were obtained, and cross-tabulations were conducted to compare results between consultants and trainee registrars, with the chi-square test used to assess significance.
Results
A total of 600 patients underwent MC over the four-year study period. The study included two consultant surgeons and eight trainee registrars, with a ratio of 1:4. Consultants operated on 58% of the cases, which included initial demonstrations for registrars and handling more complex cases. The mean age of patients was 43 years (±12.5 SD), ranging from 17 to 90. Notably, 14% (85 patients) were over 60, and registrars operated on 46.9% of these older patients. The age distribution was significantly skewed to the right. The male-to-female ratio among patients was 1:4.9. A statistically significant correlation was found between gender and operator (P = 0.049), as shown in Table 1. The distribution of operations by consultants and registrars was consistent across both genders (58% by consultants and 42% by registrars). Among patients, 10.3% (62) had comorbidities, including diabetes, hypertension, bronchial asthma, or a history of acute coronary syndrome. Registrars operated on 42% of patients without comorbidities and 45% with comorbidities. However, this difference was not statistically significant.
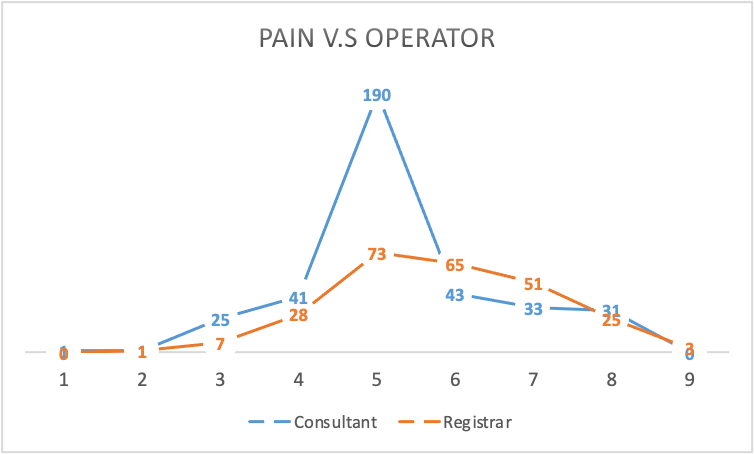
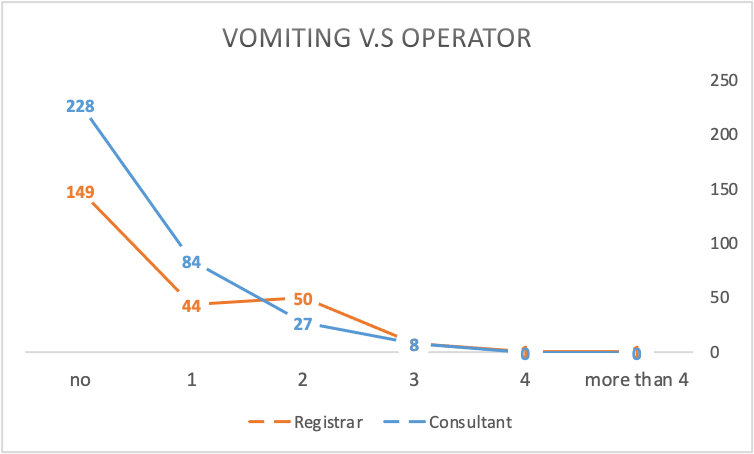
Regarding diagnosis, 49%(296) had symptomatic gallstones, 42% (250) had chronic calculus cholecystitis, 8% (48) had acute calculus cholecystitis, and 1% (6) had empyema gallbladder. Registrars operated on these cases at similar rates to consultants, with a slightly higher rate of empyema (50%) and a lower rate of acute calculus cholecystitis (37%), though these differences were statistically insignificant. The average hospital stay was 2.9 days (±0.9 SD), ranging from 2 to 15 days, including the preoperative preparation day. Table 2 shows the relationship between hospital stay duration and the operator. The percentage of operations by registrars was highest in patients with a 4-day stay (61.2%), while the average across all lengths of stay was close to 42%. This correlation was statistically significant (P < 0.0001). Biliary injury occurred in 3 patients (0.5% of total cases), all operated on by registrars. This complication rate was 1.2% among patients treated by registrars and did not occur in patients treated by consultants (P = 0.042), as shown in Table 3. Pain levels were assessed on a 0-10 visual pain scale, with a mean score of 5.4 (±1.2 SD). A small subset (3.7%) required no analgesia, while 2.2% required injectable analgesia more than three times, and only 0.7% required opioids. Registrars primarily operated on patients with pain scores of 6 or higher, and this correlation was significant (P < 0.0001), as shown in Figure 1. The number of retractors used was also analyzed for their effect on pain, showing no significant impact on pain scores despite variation from 1 to 3 retractors (P < 0.0001). Postoperative vomiting occurred in 38% of patients, with a 2.1:1 ratio favoring a higher incidence in patients operated on by registrars compared to consultants (68% vs. 32%). This correlation was statistically significant (P < 0.0001), as shown in Figure 2. Vomiting generally lasted 1-2 days postoperatively.


Discussion
This study underscores MC as a feasible and effective surgical option for gallstone disease in resource-limited settings. Given the challenges of adopting LC in LMICs due to the cost and availability of specialized equipment, MC offers a cost-effective, accessible alternative that still enables good clinical outcomes. Our findings align with research showing MC’s role as a suitable alternative where resource constraints limit access to LC, particularly in settings similar to ours in Eastern Sudan.4 One of the key insights from our study is the operative role distribution between consultants and registrars. Consultants performed 58% of the procedures, indicating their involvement in demonstrating techniques and managing more complex cases. This structured engagement of consultants supports registrars’ training and allows MC to serve as an effective educational tool in surgical training. The association between the operators and various clinical outcomes is noteworthy, particularly with statistically significant differences in patient gender and hospital stay duration. In our study, registrars performed surgeries in 46.9% of patients over 60, suggesting that MC can be adapted as a training procedure in this demographic with favorable outcomes. Additionally, this study affirms the feasibility and safety of the mini-cholecystectomy as a treatment modality and training model in surgery, which aligns with previous studies.8,9
Our patient cohort, with a mean age of 43 years, included a substantial portion of older adults (14% were over 60), suggesting that MC can be effectively performed in elderly patients, even by registrars, after adequate training. This finding aligns with previous studies reporting MC’s utility in elderly or high-risk populations due to its relatively straightforward technique, shorter operative times, and reduced anesthetic exposure, which may be advantageous for elderly patients.5,10–12
The analysis of postoperative pain revealed significant differences related to the operator. Patients operated on by registrars reported higher pain levels, with a mean visual pain score of 5.4 (±1.2 SD) and a significant correlation between pain intensity and the registrar group (P < 0.0001). This discrepancy may be attributed to variations in technical proficiency, as surgical skill often improves with experience. However, overall pain outcomes remain consistent with studies indicating that MC provides low postoperative pain intensity comparable to LC.13,14 The minimal need for analgesics, with only 2.2% requiring injectable analgesia more than three times, highlights the feasibility of MC as a minimally invasive technique regarding pain management.
Hospital stay duration was also significantly associated with the operator, with the mean stay at 2.9 days (±0.9 SD). The duration of hospital stays ranged from 2 to 15 days, and registrars tended to operate on patients requiring extended hospital stays, particularly those staying 4 days (61.2% of these cases). This correlation was statistically significant (P < 0.0001), suggesting a learning curve in postoperative management. Nevertheless, MC has shown comparable recovery times to LC in other studies, supporting its efficacy in reducing hospital stays in LMICs.15–18
Biliary injury is the most feared complication in cholecystectomy procedures; it is a key measure of surgical safety, occurring in only 0.5% of cases (3 patients), exclusively in surgeries performed by registrars. This rate of biliary injury (1.2% for registrars) underscores the potential learning curve in MC but remains low, aligning with findings that MC and LC both have rare occurrences of biliary injury with adequate supervised training.4 Importantly, no biliary injuries were reported in consultant-led surgeries (P = 0.042), reinforcing the importance of structured surgical training and experienced oversight in minimizing complications.
The study also explored postoperative vomiting, a significant finding with a higher incidence in patients operated on by registrars (68% vs. 32% for consultants; P < 0.0001). This could be attributed to subtle technical differences, though it did not affect overall outcomes. With its straightforward approach, MC enables registrars to develop fundamental surgical skills, which previous studies affirm by showing low complication rates comparable to those in LC.18 Nevertheless, this aspect highlights the need to continuously evaluate surgical techniques to minimize adverse effects, particularly in training environments. In a training unit, the trainees are expected to tend to operate in less complex cases. , The study determined the complexity of cases based on preoperative clinical assessment and ultrasound findings. Clinically, complex cases included patients with recurrent biliary colic, prolonged symptoms, a history of acute cholecystitis, or a previous abdominal procedure. Ultrasound criteria included a thickened gallbladder wall (>4 mm), pericholecystic fluid, contracted gallbladder, or impacted stones in the neck or cystic duct. Urgency is often complex, as it is acute calculus cholecystitis or empyema.
This study’s findings affirm that MC offers a comparable and often lower-cost alternative to LC, as previous studies have shown that MC reduces the need for specialized equipment and can reduce hospitalization costs due to shorter operative times and fewer postoperative requirements. This cost-effectiveness is particularly beneficial in LMICs, where healthcare budgets are constrained, and equipment limitations prevail.19–21 The overall cost savings associated with MC support its growing role as a practical alternative to LC, especially for routine cholecystectomies, as no complex, expensive surgical set-up is essential.22 Recent studies have highlighted the effectiveness of mini-laparotomy and mini-laparoscopic cholecystectomy as alternatives to traditional open and multi-port laparoscopic cholecystectomy, particularly in challenging cases or resource-limited settings. In Sudan, a 512-case study demonstrated the feasibility of mini-laparotomy cholecystectomy, achieving low complication rates and short hospital stays, proving it to be a safe and cost-effective option in resource-constrained environments.23 Another study compared laparoscopic subtotal cholecystectomy (LSTC) with open total cholecystectomy (OTC) in patients with difficult gallbladders, showing that LSTC had advantages such as reduced blood loss, shorter operative times, and a lower risk of bile duct injuries, making it a safer choice for complex gallbladder cases.24 Mini-cholecystectomy has been shown to decrease postoperative pain, enhance cosmetic outcomes, and accelerate recovery, although it requires more experience to overcome visibility challenges in complex cases.25 In evaluating MC, it’s critical to consider patient-specific factors that impact the incidence of complications. Variables like acute cholecystitis, anatomical anomalies, and previous abdominal surgeries can significantly impact surgical outcomes, irrespective of the operating surgeon’s experience. A comprehensive evaluation that accounts for these factors is crucial to accurately attribute the causes of such complications. This applies to the biliary injuries that occurred exclusively in the registrar-performed group, which may suggest a difference in outcomes between consultants and registrars. Although there were only three injuries in a sample of 600 patients, the sample size may be insufficient to detect a significant difference between the two groups. This may require a larger sample size to ensure that the observed difference is not due to random variation but represents a true disparity in surgical outcomes.26,27
Studies comparing MC and LC have given mixed results. Some research indicates that LC offers benefits of reduced postoperative pain, shorter hospital stays, and quicker return to regular activities. However, other studies suggest that MC may have advantages such as shorter operative times and lower costs.[28.29]
The results of mini-laparotomy approaches offer significant benefits for patients with complicated gallstone disease, offering suitable, safe alternatives to conventional open cholecystectomy. Our study showed the same good outcomes with the additional value of presenting a surgical training model.
Conclusions
Mini-cholecystectomy (MC) is a safe, effective, and feasible surgical option for gallstone disease in a resource-limited setting in low- and middle-income countries (LMICs). The procedure is simple and achieves favorable patient outcomes, including acceptable levels of postoperative pain, short hospital stays, and low complication rates. It also serves as an effective training tool in surgical education programs, where access to advanced laparoscopic equipment may be limited.
Study Strengths
In this study, patient selection bias was avoided by including all eligible patients. Direct observation and supervision of the outcomes enhance data reliability. As a training standard, the comparison between consultants and trainees will provide more insights into its suitability. Moreover, ethical approval and consent for participation and publication enhance the article’s credibility.
Weaknesses and Limitations
The weak points are that it’s a single-center study, on the registrar group, there are many operators, and the follow-up was limited to one year, which may overlook long-term complications. Additionally, the low incidence of bile duct injury may indicate the need for a bigger sample size to accurately evaluate this complication. There was no real randomization of the cases between consultant and registrar groups, which may include selection bias of cases.
Recommendations
-
Conduct multicenteric randomized studies with bigger sample sizes and longer follow-ups for validation of the results.
-
Enhance the training programs in LMICs and make MC a viable option when access to laparoscopic services is limited.