



Introduction
Intertrochanteric fractures, classified as extracapsular proximal femur fractures, occur in the area between the greater and lesser trochanters. They represent approximately 50% of all proximal femur fractures and are associated with significant morbidity and mortality.1 A study by Ghasemi et al demonstrated a poor quality of life in all measures, which can be improved by early surgical fixation.2
Most intertrochanteric fractures heal successfully due to their location in the metaphysis and their rich blood supply. Nonunion typically occurs as a result of suboptimal internal fixation, which can compromise the blood supply in that region because of the surgical approach used during the initial fixation.3 There are very few documented cases of intertrochanteric nonunion that occur without any prior attempts at internal fixation; these are termed “primary” intertrochanteric nonunion.
Currently, there is no established standard treatment for neglected intertrochanteric fractures. However, a valgus intertrochanteric osteotomy with dynamic hip screw (DHS) fixation appears to be the most commonly used technique for young patients, according to most literature.3–5 In contrast, arthroplasty is often recommended for older patients with severe osteoporosis or concomitant degenerative arthritis.6 Delayed presentations are frequently observed in resource-limited settings, where many patients display significant osteopenia following pretreatment with traditional herbal medications or after an extended period of disuse.7 The limited availability of implant options, combined with the technical difficulties of managing neglected and osteopenic cases, presents unique challenges in treatment.
We present 2 such cases treated at our hospital, along with the techniques employed for surgical fixation. These case reports aim to contribute to the body of knowledge regarding primary intertrochanteric nonunion and share our experiences in managing such challenging cases.
Case Presentation
Case 1
A 45-year-old man was referred to our clinic 10 months after sustaining a fall from a standing height while commuting. Initially, he received no treatment for his injury but was later admitted to another hospital, where he underwent skeletal traction for 2 months with a diagnosis of a left intertrochanteric fracture. The patient has no history of smoking or chronic medical illnesses, and he reported that he was able to walk comfortably before the incident. However, he has had a cavovarus foot deformity since childhood.
Upon examination, the patient was unable to bear weight on his affected limb, with a painful mobility at the fracture site. The left lower extremity was shortened with an externally rotated posture. Anterior posterior (AP) X-ray of the pelvis showed an ununited intertrochanteric fracture with sclerosed margins and no evidence of callus or bridging trabeculae (Figure 1). Vitamin D level was not assessed due to financial cost limitation but other labs were unremarkable, and he was admitted for surgical fixation with a diagnosis of primary intertrochanteric nonunion.

Under spinal anesthesia and in the supine position, a lateral approach to the hip was undertaken. The fibrous tissue between the fracture margins was curetted until a bleeding bony surface was reached. The reduction was achieved with traction and internal rotation of the distal fragment. For definitive fixation, a 4-hole, 135° DHS plate was used along with an 85-mm DHS screw. A valgus osteotomy was considered unnecessary as the 135° DHS plate already provided the requisite valgization to address the varus nonunion. The patient was discharged after 2 days with prescriptions for paracetamol and rivaroxaban, and he was advised to avoid weight bearing and to use crutches for ambulation.
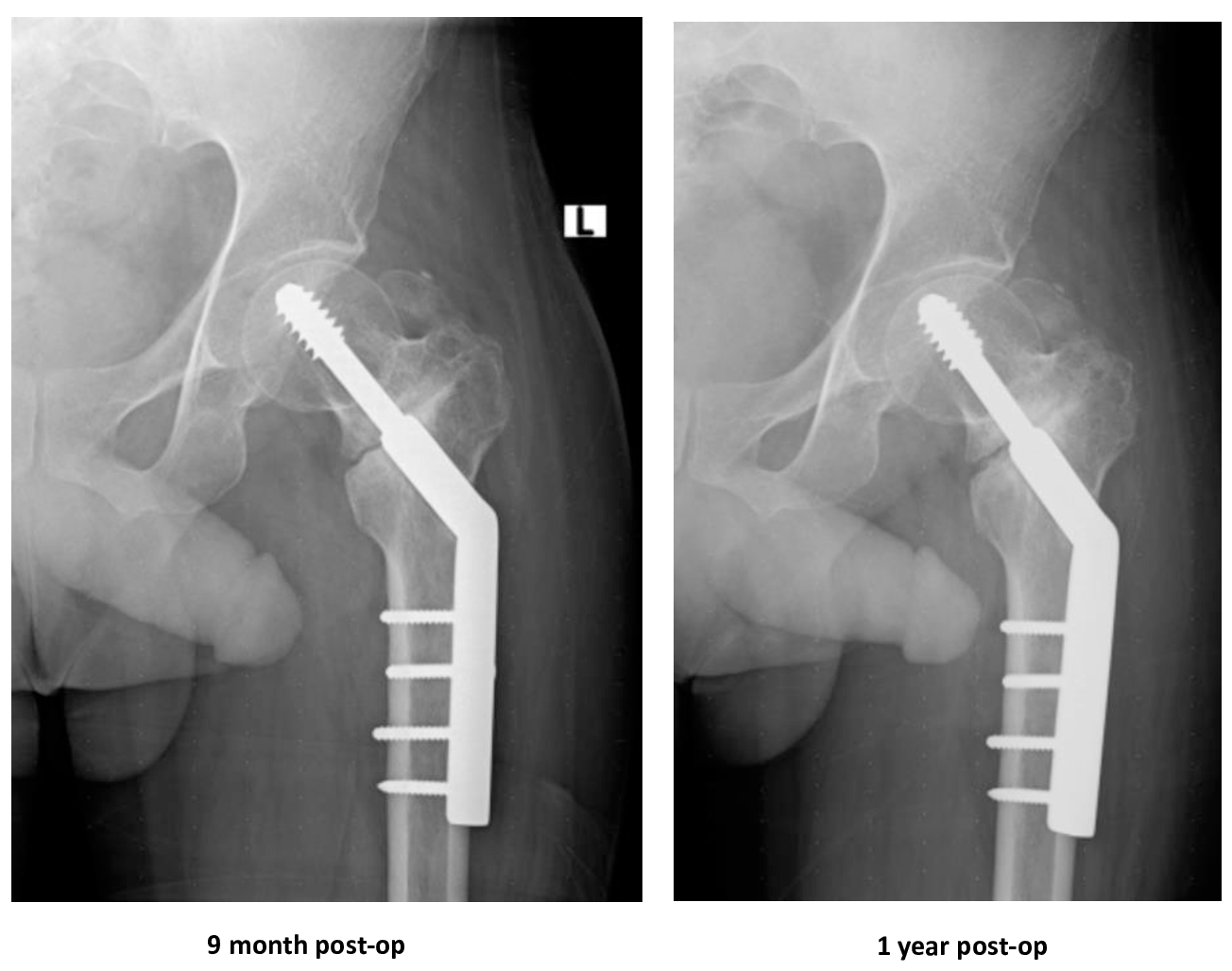
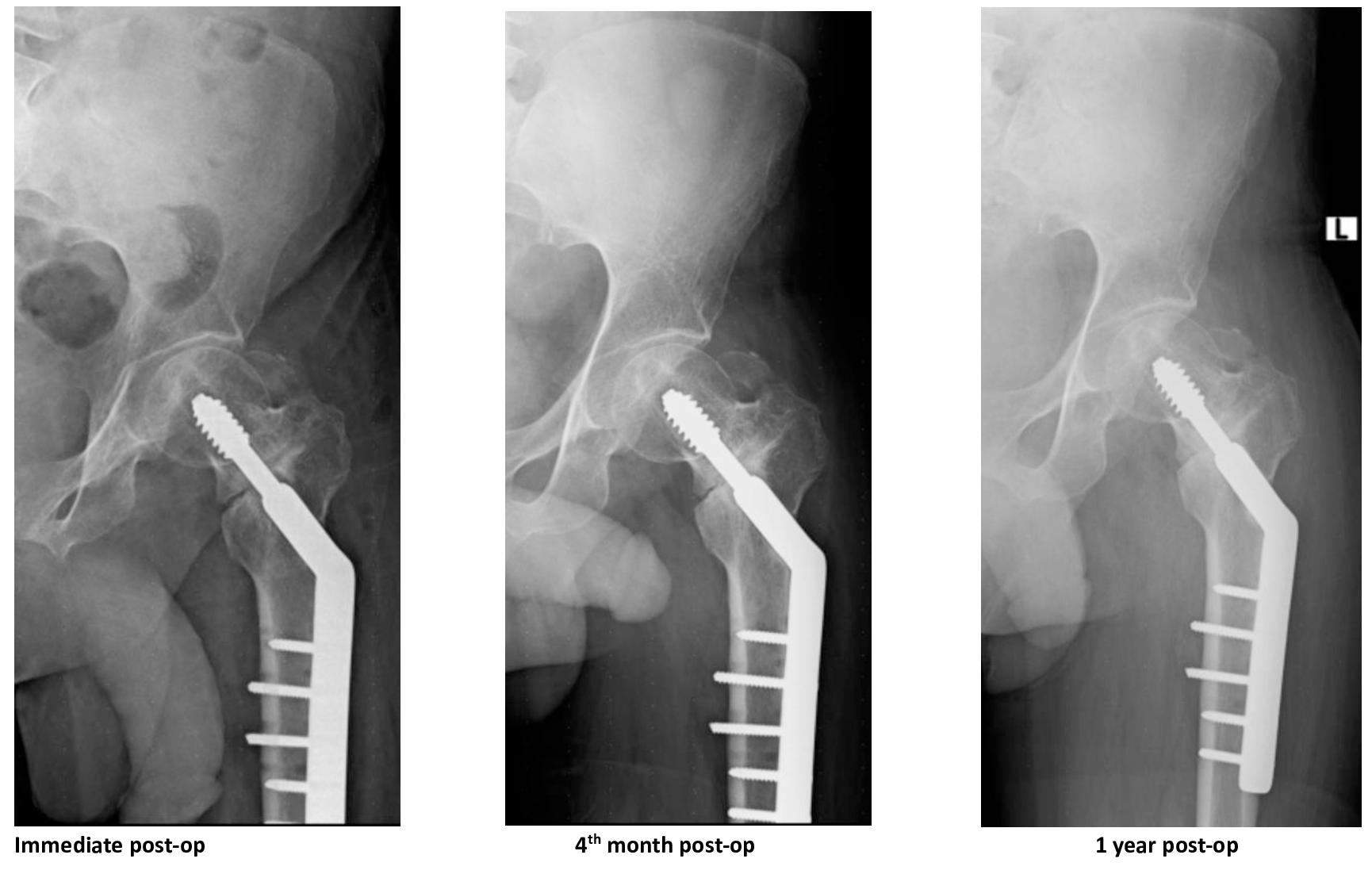
During follow-up visits, the patient failed to achieve clinical and radiological union (Figure 2). One year after the initial fixation, he was readmitted for a revision of the DHS. The previous plate was removed, the fibrous tissue was debrided, and a longer, 5-hole plate and a shorter, 80-mm DHS screw was selected. Bridging trabeculae were observed at the 4-month follow-up (Figure 3). By the 1-year follow-up, the patient reported that he could walk comfortably with minimal pain. His modified Harris Hip Score improved from a preoperative score of 26 to 80 and the patient is satisfied with his current functional status.


Case 2
A 66-year-old woman, who lives 90 km from the capital city, presented to our outpatient clinic 16 months after being struck and pushed to the ground by oncoming traffic. Initially, she sought treatment from traditional bone setters and received herbal medications. The patient has no history of smoking or chronic medical conditions and was previously able to walk comfortably prior to the incident.
On examination, her right leg was observed to be shortened, with a leg length discrepancy of 4.5 cm, and it was positioned in an externally rotated attitude. She also exhibited tenderness in the hip area. Laboratory tests yielded unremarkable results. An X-ray of the pelvis showed an intertrochanteric nonunion, characterized by rounded, blunted fracture ends and osteopenia of the right femur, with superior migration of the distal fragment (Figure 4). She was subsequently admitted for internal fixation, with a diagnosis of right primary intertrochanteric nonunion.

Under spinal anesthesia and in the supine position, we performed a standard vastus split approach. We found that the greater trochanter had migrated posterosuperiorly, along with the abductors and short external rotators. A pseudojoint, encapsulated by fibrous tissue, was identified between the neck fragment and the distal fragment. The lesser trochanter and the iliopsoas tendon were found to have migrated anteromedially. We excised all the fibrous tissue and refreshed the fracture edges until we reached a bleeding surface. Reduction was facilitated with the use of a bone clamp. A 95° blade plate was then inserted into the head and neck fragment and reduced to the shaft. We filled the gap between the axilla of the blade plate and the bone fragments with local bone graft. The split greater trochanter segment was stabilized to the main fragment using cerclage wire. The patient was discharged after 2 days with prescriptions for paracetamol and rivaroxaban. She was advised to avoid weight-bearing activities and to use crutches for ambulation. Follow-up X-rays show fixation in varus (Figure 5).

During the most recent follow-up, 16 months after surgery, it was observed that the proximal screw has become loose and palpable (Figure 6). The patient also reported difficulties in full weight bearing without crutch support. Although revision options were discussed, she has opted against any further surgical procedures. She currently has a modified Harris Hip Score of 72 and is not satisfied with her current functional status.

Discussion
Intertrochanteric proximal femur fractures are less prone to nonunion compared to intracapsular femoral neck fractures, with a reported incidence of 1%–2%.3 Diagnosis requires a fracture line to be present by 15 weeks postinjury, with either no callus formation or a callus that fails to bridge the fracture site.4 This is usually accompanied by evidence of mobility at the fracture site during examination. Most nonunion cases arise following surgical interventions that disrupt the surrounding soft tissue envelope.
Literature discussing “primary” intertrochanteric nonunion is limited. Notably, Weber and Čech reported on the first 3 cases who underwent valgization with DHS and blade plate fixation.8 Sarathy et al documented favorable outcomes in their series of 7 patients who underwent medial displacement valgus osteotomy.4 Similarly, Bartonícek reported on 2 patients who received valgization with good outcomes.5 And the largest series to date, conducted by Dhammi et al, followed 20 patients who underwent valgization and DHS fixation.3 Our report focuses on 2 patients from our institution. The first patient required revision due to failure to achieve union; however, following revision, radiological union was achieved at the 4-month follow-up, and the patient is now able to bear weight comfortably with minimal pain. The second patient continues to experience activity limitations 1 year post surgery. A 95° blade plate was chosen in this patient to preserve metaphyseal bone; however, the varus positioning and the choice of rigid fixation likely contributed to the ongoing nonunion. These 2 contrasting cases emphasize the significance of optimizing both the mechanical and biological environments in primary nonunion of intertrochanteric fractures to ensure reliable healing in these challenging surgical procedures.
Conclusion
Primary intertrochanteric nonunion is a rare and challenging injury to treat, and there is a high likelihood of failure to achieve union unless an optimal biological and mechanical environment is achieved.
Ethical Approval/Informed Consent
Formal ethical approval was not required for this case report as per institutional guidelines/local regulations for retrospective reporting of a single clinical case. Written consent for submission and publication of this case report including imaging and associated text has been obtained from the patients in line with COPE guidelines. Patient anonymity was maintained throughout the report by de-identifying all patient data.
Data Availability
Not applicable
Conflict of Interest
All authors declare no conflicts of interest.