
Background
Lower urinary tract trauma (LUTT) includes injury to the urinary bladder and urethra.1 Anatomically, the whole urinary tract system is usually protected from external forces; however, its diagnosis remains a challenge, especially in a poorly resourced setting, where radiological imaging is costly.2 In the United States, the urinary system is a significant contributor to trauma-induced morbidity and mortality, accounting for 10% of the 2.8 million people hospitalized annually due to trauma.3
A study done in Sub-Saharan Africa indicated that, of the patients admitted with urological emergencies, LUTT accounted for 88.4%.4 In children, lower urinary tract injuries accounted for 7% of all injuries, and most of them were accompanied by potentially fatal conditions such as brain, chest, and abdominal injuries.5
In Nigeria, blunt trauma due to motor vehicle crash (MVC) was the most common cause seen in 50% of lower urinary tract injuries while gunshot injuries accounted for most penetrating injuries.3 In the pediatric population, circumcision was the most common cause of urological injuries, followed by MVC.6
These injuries usually occur in the background of polytrauma and may easily be overlooked, leading to underreporting, mismanagement, and complications if not well treated.7 Therefore, this study aimed to describe the etiology, patterns, and short-term outcomes of male patients with LUTT admitted at Mbarara Regional Referral Hospital (MRRH). The objectives of this study are to describe the: (1) etiology of LUTT in male patients admitted at MRRH, (2) injury patterns of LUTT in male patients admitted at MRRH, and (3) short-term outcomes of LUTT in male patients admitted at MRRH.
Methods
Study design
This was a prospective cohort study.
Study setting and period
MRRH is a government referral and teaching hospital. The hospital is situated along the Kampala-Kabale highway. MRRH serves a population of approximately 4 million people. This hospital has a division of urology under the department of surgery. The department is headed by one urologist, who works with residents and medical officers. Patients who present with injuries of the lower urinary tract are initially evaluated at the accidents and emergency department from where a consultation with the urology team is made for specialized evaluation and management.
Participants with LUTT were admitted to the Department of Surgery of MRRH between December 1, 2022 and July 31, 2023. Follow-up was done until the time of discharge, for a maximum period of 30 days. Data collection was done from time of recruitment up to the participant’s discharge.
Study population
This study targeted male patients with LUTT admitted at MRRH during the study period. We included male patients with confirmed LUTT who consented to participate in the study. Patients who came after receiving definitive treatment from another facility were excluded because it was not possible for the study team to fully evaluate the injury. Following treatment, participants were followed up daily by taking history, clinical examination, and vitals observation until the patient’s discharge.
Recruitment, data collection procedures, and variables
Sampling was conducted consecutively for all patients who met the inclusion criteria for the study. Participants were enrolled in the order that they arrived at the hospital. Those found eligible were recruited following informed consent. For patients under 18 years, the parent or guardian gave consent. Assent was sought in addition for those between ages of 7 and 18 years. An interviewer-administered precoded questionnaire was used for data collection. A review of patient’s medical records, such as the referral form, was done where necessary. For all patients who underwent surgery, details were obtained from operation notes in liaison with surgical team. Participants underwent a full physical examination including a general physical examination, a local examination of the injury, and a thorough systemic examination. The findings were documented. The participants were followed up with until they were discharged.
The data obtained included age, mechanism and etiology of injury, organ injury, anatomic site of injury, patterns of injury, treatment modalities, and short-term outcomes of treatment. Data on etiology were collected through history taking. Social demographics of the patient were also recorded in the questionnaire. Data on injury patterns were collected through clinical examination, imaging, and intraoperative findings. Associated injuries were also documented. Short-term outcomes were collected through daily clinical evaluations done until the time of discharge.
Quality control
To determine whether the questionnaire could successfully extract the needed data on relevant variables, it underwent preliminary testing for validity and reliability at the hospital. The data collection was carried out by the principal investigator in conjunction with qualified research assistants (resident doctors) attached to the unit. The research assistants were trained on how to use the data tools. The lead investigator or his assistant doublechecked the data collection materials every day to ensure accuracy and correctness. Only those who met the inclusion criteria were recruited, which ensured the quality of the data. To ensure consistency of information when administered, the data tool/checklist was translated into local language for participants who did not speak English. Participants were selected consecutively.
Sample size
We used the formula proposed by Yamane in 1967
\[n = \frac{N}{1 + Ne^{2}}\]
From MRRH records, N = 38 (there were 38 patients with lower urinary tract injuries in the year preceding the study), e = 0.05 for a 95% level of confidence. On substitution, n = 34.7.
To improve internal validity and cater to those who could have been lost to follow-up, 10% was added, hence requiring 38 participants.
Data analysis plan
Data from retrieved questionnaires were coded appropriately into the Microsoft 2016 Excel spreadsheet and later transferred into the Stata version 15 for statistical analysis. Numerical data were summarized using medians and interquartile ranges for continuous skewed variables. Nominal data were summarized using proportions. Tables, a bar graph, and a pie chart were used to present the data. Chi-square test for categorical variables or student t tests for continuous variables were performed to determine significant differences between individual injured lower urinary tract organs. The significant level was at <5% for a 95% confidence interval. Data on etiology of LUTT were described in a pie chart and table as frequencies and percentages. The patterns of injury were described and summarized in a table as frequency and percentages. Short-term outcomes were summarized in tables with frequencies and percentages using χ2 test.
Results
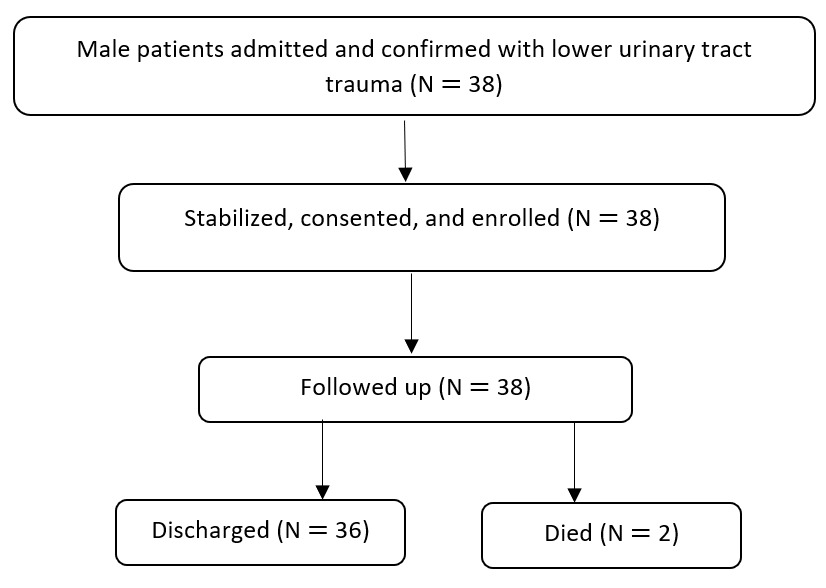
This study admitted and confirmed 38 participants with LUTT. All participants provided consent, enrolled into the study, and were followed up with until they were discharged from the hospital, for a maximum period of 30 days. Thirty-six participants were followed up to discharge; however, 2 participants died on follow-up. There was no participant lost on follow-up (see Figure 1).
The total number of lower urinary tract injuries was 50 because some participants had more than one injury. The median age of the participants was 25 years, with interquartile range 5–37 years. The majority of the participants were peasant farmers (n = 25, 65.8%). Most participants attained primary education (n = 20, 52.6%; see Table 1).
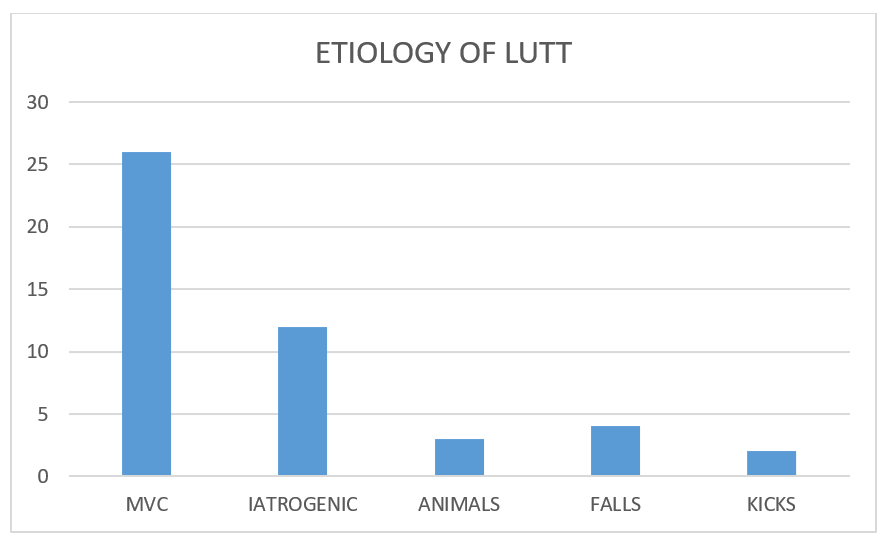
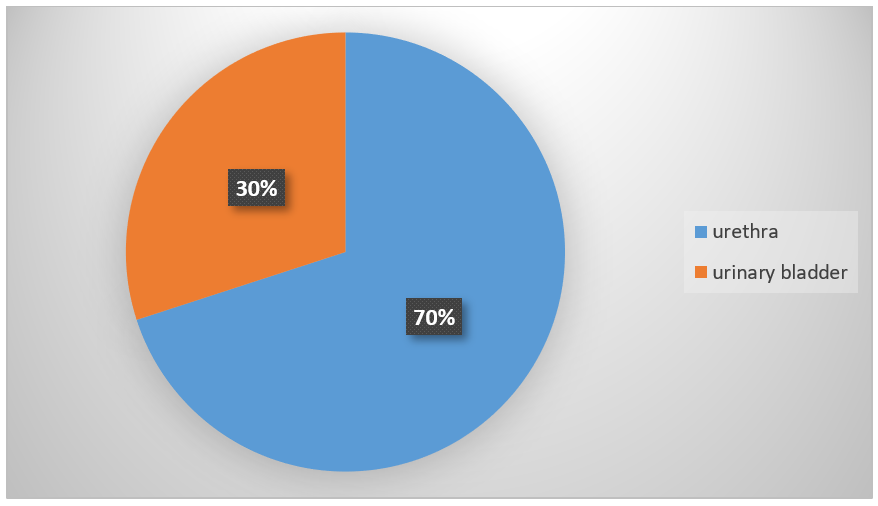
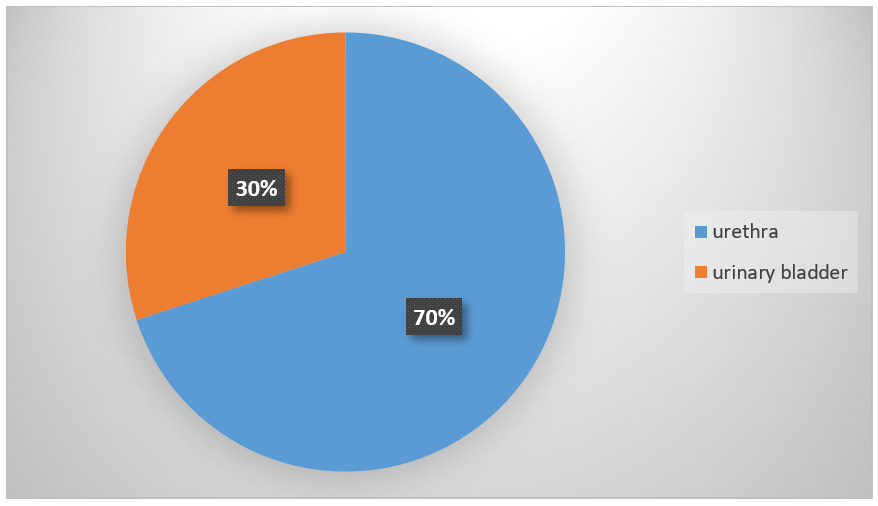
MVC was the most common etiology of LUTT (52%), due to motorcycle transport system, followed by iatrogenic injuries (24%; see Figure 2). The urethra was the most injured organ (70%; see Figure 3). Urethra complete tear was the most common urethra injury pattern (62.9%; see Table 2).

Mortality occurred in 2 of the participants (5.3%); these participants were also associated with head injuries. A majority of the participants with LUTT stayed in the hospital longer, for a period of over 1 week (65.8%). Generally, the complication rate following treatment was high (64.1%), and urethral bleeding was the most common complication (36.8%; see Table 3).
Discussion
LUTT is a significant contributor to trauma-induced morbidity and mortality by posing a significant public health challenge once it happens. It rarely occurs in isolation and is always associated with injuries to other vital organs. We prospectively recruited participants to describe the etiology, patterns, and short-term outcomes of LUTT in male patients admitted at MRRH.
In this study, 38 participants were enrolled. The median age was 25 years; this was similar to studies done in Kenya by Oluoch, in which their median age was 28 years.7 This is explained by similar environmental and participant characteristics in which both countries are still developing. Most of our population is characterized by youth who usually get involved in aggressive sports, the motorcycle transport business without obeying traffic rules, and other risky behaviors (eg, substance use). Similar findings were also observed by Furr et al in Nigeria.8
Injuries to the lower urinary tract organs occur as a result of blunt, penetrating, or iatrogenic trauma. In this study, most of the lower urinary tract injuries happened as a result of MVC. Similar findings were reported by Oluoch7 at Kenyatta National Hospital and in Nigeria by Ahmed et al9 where motor vehicle accidents were the most common cause, accounting for 47.5% and 68%, respectively. This could be explained by similar environmental characteristics where the majority of the population in Sub-Saharan Africa gets involved in the commercial motorcycle transport business, in which most of the traffic regulations are not observed. Iatrogenic injuries due to circumcision (20.5%) were observed to be the most common cause of urethra injuries in our setting, similar to a report in Nigeria by Osuigwe et al.6 This could be explained by the fact that some people in our communities still have circumcision done by cultural and religious groups of people. These people are not surgically trained and are not supervised throughout their practice, leading to genital injuries. A similar issue has been observed in low cadre health workers practicing at lower health facilities with no experience in pediatric circumcision. Similar findings were observed by Barry Mi et al in Guinea.(1)
LUTT includes injuries to the urinary bladder and the urethra. In this study, the urethra was the most injured organ. This is similar to the studies done in Kenya in which urethral injury accounted for 51.9%.7 This could be explained by a similar etiology (MVC).
In this study, extraperitoneal bladder contusion with hematoma was the most common injury pattern. This is in agreement with studies done in the United States by Phillips et al, which showed that extraperitoneal bladder injuries were the most common (63%) compared to intraperitoneal bladder injuries.10 This could have been explained by similar etiologies of bladder injuries in which MVC was the most common cause
In our study, complete tear of either the anterior or posterior part of the urethra was the most common injury pattern. This was similar to the studies done in the United States by Patel et al, in which 65% of urethra injuries were complete tear.11 This is could be explained by similar etiology of injuries in which most of urethra injuries were due to blunt trauma as a result of motor vehicle crash.
Following treatment of LUTT, a majority of participants stayed in the hospital for more than 1 week (25, 65.8%), which could be explained by associated injuries and high complication rate in our participants. Similar studies were observed in the United States where their average length of hospital stay was 9 days due to concomitant associated injuries (Abel, 2012).(17) n this study, mortality was 5.3% (n = 2), all of whom had intraperitoneal bladder ruptures and also associated severe injuries, which could have explained death in our setting. This is different from studies done in the United States, where mortality was at 16%.12 This could be explained by differences in etiology where most of their injuries were due to penetrating injuries as a result of gunshot. An overall complication was (22, 57.9%). Similar studies were documented at a teaching hospital of Treichville, Abidjan, Cote d’lvoire at 34%.13
Bleeding per urethra was the most common complication following treatment (14, 36.8%). This could be explained by the robust blood supply of the urethra and other pelvic organ system, which is worsened by associated unstable pelvic fractures despite urinary diversion. Different studies were documented in United States, where the complication rate was lower at 15%14 and 32%.15 This could be explained by a better US health care system where most of the LUTT is diagnosed early and endoscopic procedures are done such as urethral realignment.
Study limitation
The follow-up in this study stopped at discharge; therefore, any complications that occurred later, such as strictures, were not considered in this study. However, the findings in this study will be used to design a study with a longer follow-up.
Conclusion
MVC due to motorcycle transport system is the leading cause of LUTT. The urethra is the most injured organ, and urethral bleeding is the most common complication following treatment. Among the pediatric population, circumcision was the most common cause of urethra injury, hence laws should be put in place for pediatric circumcision to be done by a trained and qualified health personnel.
Acknowledgments
I take this opportunity to acknowledge my wife RA and my daughter AAC.
Ethical Approval
All methods were carried out in accordance with relevant guidelines and regulations. Ethical approval was granted by the Research and Ethics committee of Mbarara University of Science and Technology (Ref No: MUST-2023-770).
Informed Consent
All participants gave written, informed consent as evidenced by the participants’/guardian’s signature. Informed consent to participate was obtained from the parents or legal guardians of any participants under the age of 18.
Data Availability
Data is available upon request. Requests should be sent to 0785011339a@gmail.com.
Conflict of Interest
The authors declare that they have no conflict of interest
Funding
None.