
Introduction
The pituitary gland, or the “hypophysis cerebri,” located within the sella turcica, is a critical endocrine organ often referred to as the “master gland” due to its regulatory role in numerous physiological processes. Pituitary adenomas, benign tumors arising from the gland, account for 10%–20% of intracranial neoplasms, with adenomas representing 90%–95% of these cases.1–3 These tumors are classified based on size as microadenomas (<10 mm), macroadenomas (≥10 mm), or giant adenomas (≥40 mm), and their clinical presentation varies depending on hormonal activity and mass effect.4 Clinically, pituitary adenomas can be classified as hormonally active or functional, and hormonally inactive or nonfunctional. Radiologically, pituitary adenomas can be classified based on the Hardy grading system which factors in the size and invasiveness of the tumor.5 This system was later modified by Wilson to incorporate different grades of extrasellar extension.6 Cytologically, the cells of the adenohypophysis and their corresponding tumors can be classed based on their staining properties on light microscopy into acidophils (somatotrophs and lactotrophs), basophils (thyrotrophs, corticotrophs, and gonadotrophs), and chromophobes. Chromophobes exhibit no staining because they have minimal to no hormonal content. They are thought to be undifferentiated stem cells (from Rathke’s pouch) which give rise to plurihormonal adenomas. Both acidophils and basophils are grouped as chromophils.7,8 Though largely now overtaken by newer classification systems, the cytological basis remains relevant in describing the tumor behavior, especially when utilized in conjunction with other classification tools.
Pituitary apoplexy, a severe complication of adenomas, involves hemorrhage or infarction of the tumor or gland, leading to acute symptoms such as visual disturbances, altered mental status, and hypopituitarism. Though it more often complicates a pituitary adenoma, it can occur in a normal pituitary gland.9 When untreated, mortality is as high as 45%.10 While the exact mechanisms remain unclear, risk factors that have been associated with pituitary apoplexy include tumor size, vascular compromise, prior major surgery, brain injury, angiographic procedures, bleeding disorders, cardiovascular comorbidities (diabetes, hyperlipidemias, hypertension), some medications (including antiplatelets and anticoagulants, aspirin) and pregnancy (postpartum pituitary necrosis or Sheehan’s syndrome).11–15 The risk of hemorrhage in pituitary adenoma is known to be relatively high compared to other intracranial tumors, with rates as high as 9.5%–15.8%.16–18 The risk is higher in patients with undiagnosed pituitary adenoma—up to 65%.19 The exact mechanism of pituitary apoplexy in a pituitary adenoma is little known. Two patterns of apoplexy can be observed—apoplexy involving only the adenoma while sparing the normal gland, and apoplexy involving the entire gland.16,17,20 For the first pattern, it is thought that the adenoma outgrows its blood supply and ability of the body to initiate sufficient angiogenesis to sustain the tumor. In such precarious state, any condition or procedure which either reduces blood supply to the gland (eg, systemic hypotension) or increases the metabolic demands of the gland inclusive of the tumor (eg, angiographic procedure), will likely precipitate an apoplexy. The resultant ischemia leads to necrosis and hemorrhage. The second observed pattern is usually seen with macroadenomas and giant adenomas. In this scenario, growth of the tumor causes compression of the pituitary stalk, resulting in compromise to the superior hypophyseal supply along the stalk enroute the anterior lobe. This results in ischemia, necrosis, and hemorrhage of both the normal and pathological portions of the anterior lobe. The clinical manifestations result from a combination of pressure effects of the expanding sellar from the hemorrhage on the pituitary and surrounding structures, including the optic apparatus, hypothalamus, leakage into the subarachnoid space, and ventricles. Corticosteroid deficiency can be especially life-threatening, as such, steroid replacement should be a priority. Diagnosis of pituitary apoplexy is made by a combination of these clinical manifestations (especially when a prior diagnosis of pituitary adenoma is known) with radiologic findings of a pituitary adenoma with hemorrhagic and necrotic components on magnetic resonance imaging (MRI) or computed tomography scan. Definitive diagnosis is by histology following resection.
Initial management of a pituitary apoplexy remains somewhat controversial. It was previously considered a neurosurgical emergency but current trends point to increasing positive outcomes following initial conservative approach.16,21–23 Furthermore, studies had demonstrated that emergent surgery done for pituitary apoplexy resulted in recovery of up to 94% of visual symptoms compared to only 23% improvement in endocrinological symptoms.24–27 Thus, surgery is generally reserved for those with severely impaired or progressively worsening visual impairment, or those with worsening level of consciousness despite initial conservative approach.28 Better outcomes with surgery are obtained in those who are operated early (within 8 days).28 Appropriate timing to surgery is a key component to achieving better prognosis and outcome. Therefore, such patients who meet the indication for surgical intervention should be promptly identified, as this could be potentially lifesaving, and in addition, reduce the risk of permanent neurologic disability.
This study investigates the correlation between pituitary adenoma size, cytological characteristics, and the risk of apoplexy, aiming to refine risk stratification and guide clinical management.
Methods
This retrospective cohort study was conducted at a single tertiary neurosurgical center over a 3 year period. Patients were included if they were aged 16 years or older and had histologically confirmed pituitary adenomas that underwent surgical resection. Exclusion criteria comprised of nonadenomatous sellar lesions, incomplete medical records, or absence of preoperative MRI imaging. Participants were identified through consecutive sampling from the hospital’s neurosurgical database, ensuring a representative cohort.
The primary outcome was the occurrence of pituitary apoplexy, diagnosed through a combination of radiological evidence (1.5T MRI showing hemorrhage or infarction) and intraoperative confirmation. Tumor size was categorized as microadenoma (<1 cm), macroadenoma (1–4 cm), or giant adenoma (>4 cm) based on preoperative MRI measurements. Histopathological subtypes (acidophil, basophil, chromophobe, nonspecific) were determined postoperatively using light microscopy and staining techniques. Additional variables collected included demographic data (age, sex), presenting symptoms (visual loss, headaches, endocrine dysfunction), and Hardy-Wilson and modified Knosp-Steiner grading systems for invasiveness. For clarity and consistency, we primarily employed the Hardy-Wilson classification and the modified Knosp-Steiner grading system in this study. While other grading systems exist, these 2 were selected as they directly assess tumor size, sellar invasion, and cavernous sinus involvement, which were central to our analysis. All references to grading in this manuscript have therefore been standardized to Hardy-Wilson and Knosp-Steiner throughout.
To address potential biases, 2 independent radiologists reviewed all MRI scans, with discrepancies resolved by a third senior radiologist. Intraoperative findings were documented by the surgical team. Statistical analysis was performed using SPSS version 26.0. Categorical variables were compared using χ2 tests, while logistic regression assessed the association between tumor size/histopathology and apoplexy, adjusting for age and sex. A P value < 0.05 was considered statistically significant. Missing data were minimal (<5%) and handled via pairwise deletion.
Results
Our study cohort comprised 57 patients histologically diagnosed with pituitary adenomas, among which 23 (40.4%) developed pituitary apoplexy, as confirmed by both radiological and intraoperative findings. The demographic analysis revealed a higher prevalence of pituitary adenomas in the age group of 46–60 years (43.9%) and a male predominance (59.6%) (Table 1).
The majority of adenomas were macroadenomas (94.7%; 54 cases), with giant adenomas (>4 cm) constituting nearly half of the cases (49.1%; 28 cases). Microadenomas constituted 5.3% (3 cases) and tumors between 1–4 cm in sizes constituted 45.6% (26 cases).
The primary symptoms at presentation were progressive visual loss in 87.7% of cases, followed by headaches (7%), and endocrine symptoms (5.3%) (Table 2). A detailed breakdown by tumor size showed that all patients with macroadenomas (1–4 cm) and the majority of those with giant adenomas (>4 cm) presented with progressive visual loss. Headaches occurred exclusively in giant adenomas (14.3%; N = 4), while endocrine symptoms were limited to microadenomas (100%; N = 3).
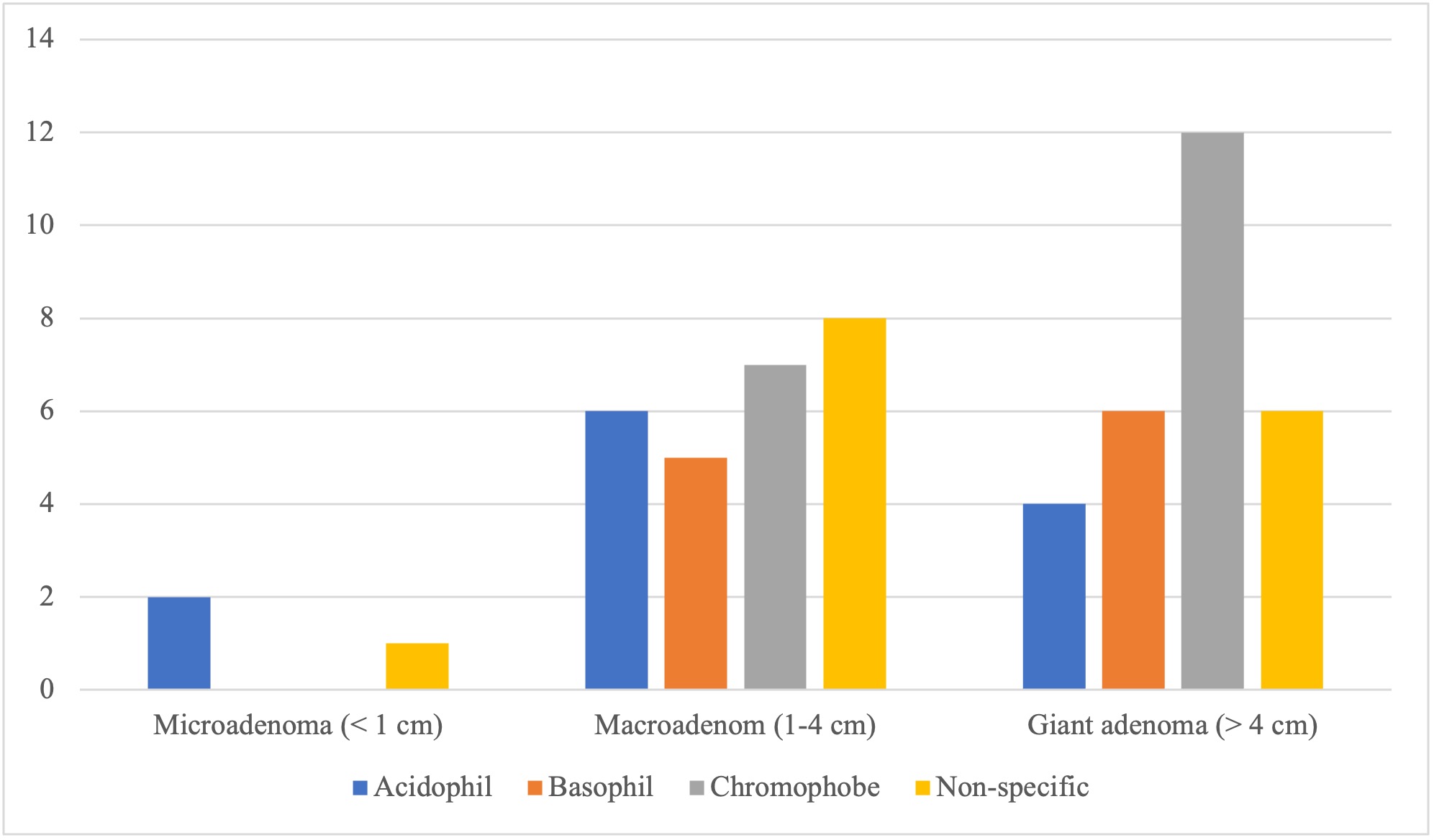
Cytological analysis identified chromophobe adenomas as the most prevalent type (33.3%, N = 19), followed by acidophilic and basophilic adenomas (Table 2).
The correlation between tumor size and cytological type was particularly notable, with chromophobe adenomas predominantly associated with larger tumor sizes (Figure 1).

Our statistical analysis demonstrated a significant positive correlation between the size of pituitary adenomas and the occurrence of apoplexy (P = .040), with giant adenomas showing the highest risk of apoplexy (odds ratio, 3.2; 95% CI, 1.1–9.4) (Figure 2), and chromophobe subtypes exhibiting a trend toward increased apoplexy incidence (52.6%; N = 10). Hardy-Knosp grading revealed that tumors with cavernous sinus invasion (Grade 3B–4) had lower gross total resection rates (64% vs 85% in Grade 0–2). This suggests that tumor size is a critical factor in the development of pituitary apoplexy.

Sensitivity analyses excluding nonspecific subtypes (N = 16) reinforced the association between tumor size and apoplexy (P = .032). No significant confounding by age or sex was observed in adjusted models.
Discussion
Demographics and clinical presentation
The demographic profile of our study cohort revealed a predominance of pituitary adenomas in patients aged 46–60 years (43.9%), with a male preponderance (59.6%). This aligns with existing literature suggesting a higher incidence of pituitary adenomas in middle-aged individuals and a slight male bias, particularly in nonfunctioning adenomas.29,30 Disruption of the hypothalamo-pituitary axis tends to be clinically evident earlier in females than in males.31 Thus, most functional pituitary tumors tends to manifest earlier in females than males, and females correspondingly tend to present for treatment earlier than males. The high prevalence of apoplexy (40.4%) in our cohort underscores the critical need for early recognition and intervention, as apoplexy can lead to life-threatening complications such as acute hypopituitarism and visual impairment.
The primary presenting symptom in our cohort was progressive visual loss (87.7%), which was almost exclusively observed in patients with macroadenomas (1–4 cm) and giant adenomas (>4 cm). This finding highlights the role of tumor size in exerting mass effect on the optic chiasm, a well-documented phenomenon in larger adenomas. In contrast, endocrine symptoms were solely reported in patients with microadenomas (<1 cm), reflecting the functional nature of smaller adenomas, which often present with hormonal hypersecretion rather than mass effect. Headaches, though less frequent (7%), were exclusively associated with giant adenomas, likely due to dural stretching or elevated intracranial pressure.
Tumor size and apoplexy risk
Our study demonstrated a statistically significant correlation between tumor size and the risk of apoplexy (P = .040), with giant adenomas (>4 cm) exhibiting the highest risk. This significant correlation between tumor size and the occurrence of apoplexy adds valuable evidence to the ongoing debate on the pathophysiological mechanisms underlying apoplexy. Our observation in this study supports the hypothesis that larger tumors are more susceptible to vascular compromise due to their disproportionate growth relative to their blood supply. The resultant ischemia and necrosis predispose these tumors to hemorrhage and infarction, culminating in apoplexy. Furthermore, while vascular compromise has been widely accepted as a key factor, our study suggests that the mechanical stress exerted by larger tumors on the pituitary gland’s vasculature may also play a crucial role. The modified Hardy-Wilson grading system and Knosp-Steiner grading (Table 3), which incorporates tumor size and invasiveness, provides a framework for understanding this relationship. Giant adenomas, by virtue of their size, are more likely to compress the pituitary stalk, disrupting the superior hypophyseal blood supply and precipitating apoplexy. This mechanistic explanation is further corroborated by the high frequency of apoplexy in our cohort, particularly among patients with macroadenomas and giant adenomas.
Cytological characteristics and tumor behavior
Cytological analysis revealed that chromophobe adenomas were the most prevalent subtype (33.3%), followed by acidophilic (21.1%) and basophilic (17.5%) adenomas. Chromophobe adenomas, which are typically nonfunctional, were disproportionately associated with larger tumor sizes. This finding is consistent with the notion that nonfunctional adenomas often remain clinically silent until they attain considerable size, at which point they present with mass effects or apoplexy.32 Our findings regarding the predominance of chromophobe adenomas and their association with larger tumor sizes are consistent with existing studies that have also reported a similar distribution of pituitary adenoma subtypes.33–35 The predominance of chromophobe adenomas in our cohort may also reflect their aggressive growth behavior, as these tumors are thought to arise from undifferentiated stem cells with a propensity for rapid proliferation.32 In contrast, acidophilic and basophilic adenomas, which are often functional, tend to be diagnosed earlier due to hormonal symptoms, thereby limiting their growth potential.32 This cytological stratification not only aids in prognostication but also underscores the importance of histopathological evaluation in guiding clinical management.
Clinical implications and management strategies
The high incidence of apoplexy in our study underscores the need for heightened vigilance in patients with larger adenomas. Given the significant morbidity associated with apoplexy, early surgical intervention should be considered in patients with severe or progressive visual deficits, as delayed treatment can result in permanent neurological sequelae. However, the role of conservative management in stable patients cannot be overlooked, particularly in cases where endocrine stabilization and close monitoring suffice.
Our findings also highlight the importance of preoperative risk stratification based on tumor size and cytology. For instance, patients with giant chromophobe adenomas may benefit from more aggressive surveillance and timely surgical intervention to mitigate the risk of apoplexy. Conversely, microadenomas with endocrine symptoms may be managed medically or with targeted surgical resection, as their risk of apoplexy is comparatively lower.
Limitations
This study is limited by its retrospective design and the relatively small sample size, which may restrict the generalizability of our findings. Additionally, the absence of long-term follow-up data precludes an assessment of postoperative outcomes and recurrence rates. Future prospective studies with larger cohorts are warranted to validate our observations and explore the interplay between cytological subtypes, tumor size, and apoplexy risk in greater depth.
Conclusion
Our study demonstrates that tumor size and cytological characteristics are critical determinants of apoplexy risk in pituitary adenomas. Giant adenomas, particularly those of the chromophobe subtype, are associated with the highest risk of apoplexy, necessitating prompt clinical and surgical intervention. These findings advocate for a tailored approach to management, integrating radiological, cytological, and clinical parameters to optimize patient outcomes. Further research is needed to elucidate the molecular mechanisms underlying these associations and to refine risk stratification protocols.
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Board of Memfys Hospital for Neurosurgery, Enugu.
Informed Consent
This study involved a retrospective review of anonymized patient records. The Institutional Review Board of Memfys Hospital for Neurosurgery approved the study and determined that individual informed consent was not required.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request. Patient-level data are not publicly available due to privacy and confidentiality restrictions.
Conflict of Interest
None
Funding
None