
Introduction
Enterocutaneous fistula (ECF) is commonly seen in the postoperative period. A few cases have been noted to occur as a result of femoral hernia strangulation. Femoral hernia occurrence in men accounts for less than 5% of the abdominal wall hernias, compared to 20% in women.1 The hernia commonly strangulates; however, the formation of an ECF from a femoral hernia is rare.
As a type of groin hernia, femoral hernia in males has an incidence of 5% among the abdominal wall hernias, compared to a 20% incidence in females.1 It passes through the femoral ring, a narrow passage, which predisposes the hernia contents to strangulation.2 For all strangulated hernias, a Richter’s hernia accounts for about 5%–15%, with more elderly patients being affected more compared to other age groups. It has a mortality rate estimated at 17%.3 A fecal fistula, or an ECF, commonly occurs in the postoperative period, especially after a hernia mesh repair of a strangulated hernia, or after procedures performed due to inflammatory bowel disease or malignancies.4 Spontaneous fistulas occur as a result of diverticulitis, radiation, Crohn’s disease, intestinal tuberculosis, appendicitis, enteric fever, and strangulated inguinal and femoral hernias. Very few ECFs from a femoral Richter’s hernia have been reported. We encountered a case of ECF from a femoral Richter’s hernia. As this is a rare entity, it is being reported.
Case Presentation
WJ, a 45-year-old male, presented to the Outpatient General Surgery Clinic at Meru Teaching and Referral Hospital with a history of foul-smelling greenish feculent discharge from the right inguinal region for three years. The discharge had started spontaneously following a painful inguinal swelling that had been present for a week. He reported some pain relief after the swelling burst. He had no history of nausea, vomiting, hotness of body, abdominal distention, or colicky abdominal pain. He was able to open bowels.
At presentation, his vital signs were normal. There was no evidence of peritonitis or abdominal distention on abdominal examination. Digital rectal examination was unremarkable. He had an ECF in the right groin, below the inguinal ligament. The fistula was discharging greenish feculent material. The patient had no evidence of sepsis. Examination of the left groin was unremarkable.
The patient was admitted for an elective hernia repair. A pelvic ultrasound reported a right inguinal hernia. Laboratory investigations, including a complete blood count and kidney function tests, were all within the normal range.
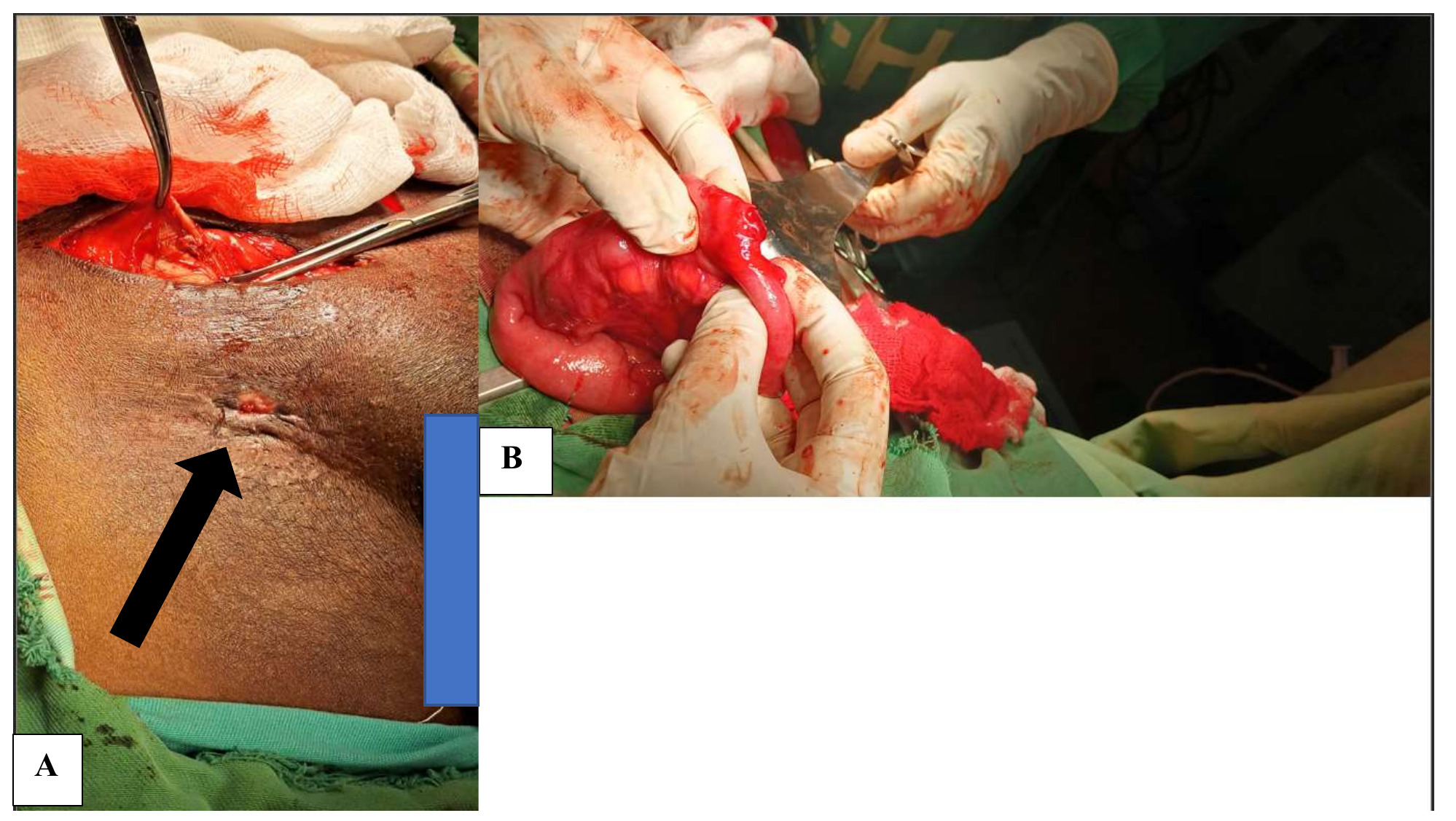
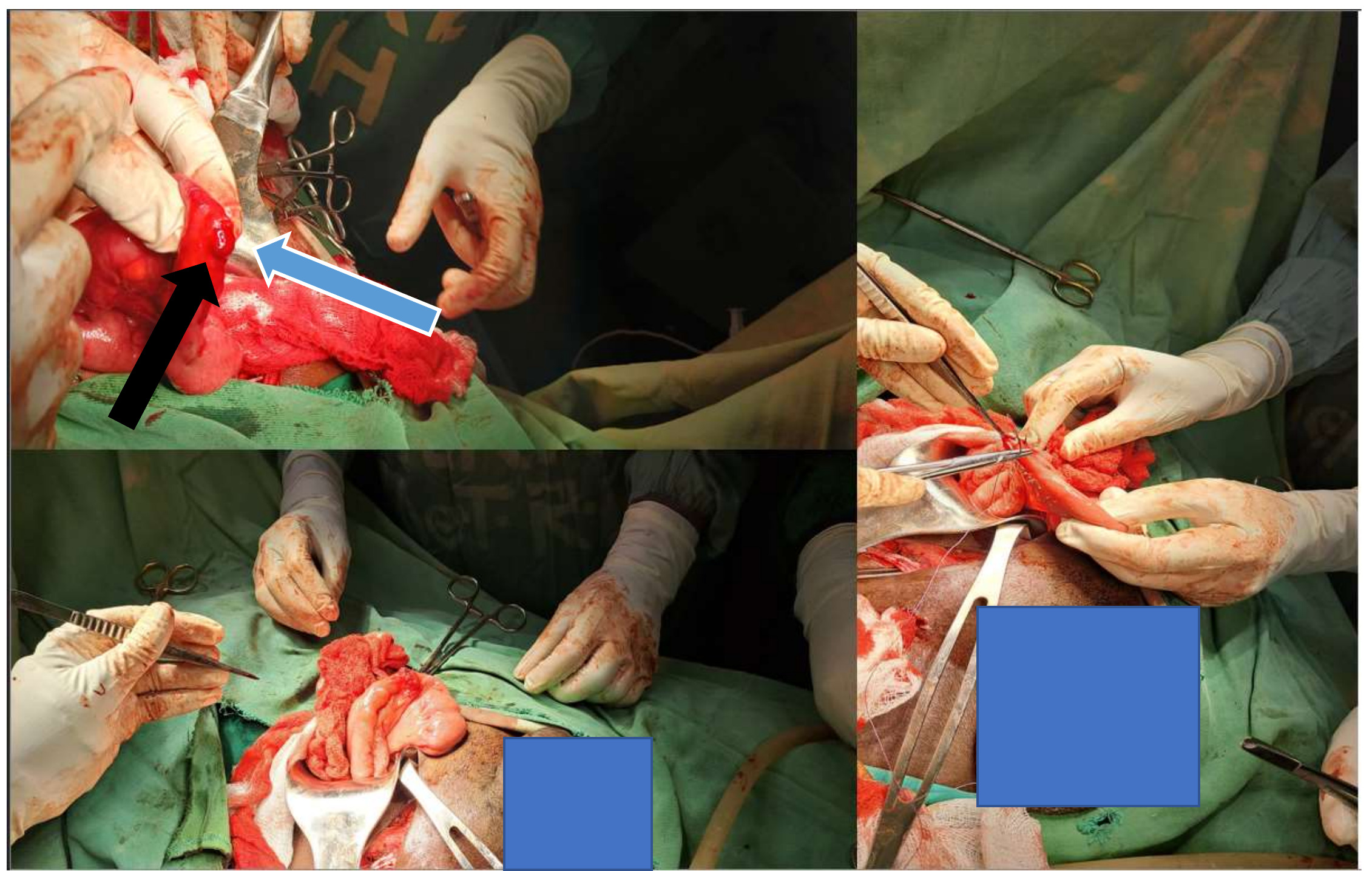
The patient was diagnosed with an ECF likely from a longstanding complicated groin hernia. He consented to an elective hernia repair and a possible exploratory laparotomy. Initial exploration was done via the inguinal crease incision, with notable findings of an intact right internal inguinal ring and a posterior wall, ruling out an inguinal hernia. Upon further exploration of the femoral canal below the inguinal ligament, a strangulated femoral hernia sac with extensive adhesions and fibrosis with a fistulous tract was noted. A lower midline incision was made. While still under general anesthesia, exploration of the abdomen was done to help reduce the hernia contents. The patient had a portion of the small bowel loop trapped within the femoral canal, 15 cm from the ileocecal junction, with an ECF, less than 50% of the circumference. The bowel loop was released, a wedge resection of the fistulous tract was done, and primary repair was done in two layers. The femoral ring was repaired primarily with a nylon 2/0 suture. The repair of the inguinal canal was performed. The inguinal ligament was approximated to the pectineal ligament. The skin defect was also repaired after resecting the cutaneous fistula. The abdomen was closed in layers (Figures 1 and 2).
_enterocutaneus_fistula_(black_arrow)_and_(b)_released_portio.png)
_the_fistula__50__of_the_small_bowel_circumference_(blue_arro.png)
The patient had an uneventful postoperative period and was discharged on day 5 post-op. There were no post-op complications. On subsequent reviews, he had developed a superficial surgical site infection, likely due to the contaminated nature of the surgery. Overstayed sutures may have aggravated the surgical site infection by acting as a nidus and scaffold for biofilm formation, thereby facilitating bacterial multiplication and subsequent infection at the surgical site. For this patient, there was a role of delayed primary closure in reducing the surgical site infection (SSI) rate because the presence of a fistula already contaminates the wound. A randomized controlled trial showed a significant reduction in SSI rates following delayed primary closure.5 The sutures were removed, with alternate-day cleaning and dressing. The wound has subsequently healed well (Figure 3). The patient was happy with how he was managed and the outcomes. He gave a written informed consent for the publication of this case report.
__and_the_healed_inguinal.png)
Discussion
An ECF is a connection between the gastrointestinal tract and the skin. Classification depends on the organ of origin, etiology, and physiology.6 The incidence of ECF is estimated at 2.3 per 100,000 persons every year.7 An ECF has an increased morbidity and mortality for patients due to the potential for infection and malnutrition that may lead to death.7 Based on the total output, ECF can be classified as a high-output, moderate-output, or low-output fistula. A high-output fistula has an output OF >500 mL/24 h, a moderate output has between 200–500 mL/24 h, and a low output is <200 mL/24 h. Most ECFs are iatrogenic, accounting for 75%–85%, while 15%–25% occur spontaneously. In our case, the ECF occurred as a result of a right femoral Richter’s hernia.
Femoral hernias occur as a result of protrusion into the femoral canal of abdominal pelvic contents. It is a rare form of groin hernia, accounting for about 2%–4% of the three common groin hernias.8 It occurs in both males and females; however, it is more common in females. A femoral hernia will commonly have a segment of bowel herniating through the canal. This type of hernia is mostly known as Richter’s hernia. It involves the protrusion and/or strangulation of only a part of the intestines’ circumference, mostly the antimesenteric side.9 The hernia may rapidly progress to strangulate and become gangrenous because the constricting femoral ring compromises the blood flow by exerting pressure on the walls of the bowel loops.2 Due to involvement of less than two-thirds of the bowel wall, features of intestinal obstruction are absent. Consequently, bowel wall ischemia is diagnosed late. Our patient had the antimesenteric portion of the bowel in the femoral ring, hence a Richter’s hernia. This type of hernia was first described in 1785 by a German surgeon, August Gottlieb Richter, and was subsequently named after him.3,10 As compared to other strangulated hernias, Richter’s hernias are commonly associated with necrosis of the bowel wall.10 It commonly occurs on small hernial defects such as the inguinal canal and femoral ring, affecting elderly patients more; however, it can occur at any age.3 As for this case, the patient was a 45-year-old male. Various case reports have highlighted the different presentations of Richter’s hernia, showcasing the diagnostic difficulty due to incomplete luminal obstruction.
In our case, the patient had an ECF as a result of chronic strangulation with the absence of luminal obstructive symptoms. The exploration was through a lower midline incision due to the presence of an ECF after bowel perforation from strangulation.
Management of ECF follows the SNAP (sepsis, nutrition, anatomy, procedure) guidelines. It requires aggressive management of sepsis, electrolytes and renal function, fluids, metabolic support, and fistula output management.11 The patient is first resuscitated, then sepsis is identified as a result of intra-abdominal infection. This is followed by defining the anatomy of the fistula using imaging techniques. A computed tomography augmented with water-soluble contrast administered orally, or through the fistula tract, provides a survey of the anatomy.12 After the initial stages of the SNAP guidelines, the ECF is surgically treated electively. In the case presented, the patient had the ECF for three years, during which time the fistula had matured, and corrective surgery was necessary.
Conclusion
ECF from a femoral Richter’s hernia is a rare occurrence. It mostly involves the antimesenteric side of the bowel, and though it has a high risk of strangulation, it will rarely have obstructive symptoms due to involvement of only a part of the bowel circumference. Most of the patients seen in our facility lack the appropriate knowledge level required to make a timely consultation. This may contribute to complications like fistula formation. Even with the delayed presentation, management of such cases is still possible by following the protocols, as in our case.
Ethical Approval/Informed Consent
Well informed consent was obtained from the patient for purposes of presenting their case for publication.
Data Availability
Not applicable
Conflict of Interest
None
Funding
None