Introduction
Abdominal surgery is an essential procedure used to treat a wide range of conditions. However, it comes with serious risks; one of the most significant being surgical site infections (SSIs). These infections not only increase the morbidity but also lead to prolonged hospital stays and higher health care costs.1–4 SSIs, defined by the Centers for Disease Control and Prevention (CDC) as infections occurring within 30 days postoperatively (or 1 year in case of an implant),5 vary in prevalence depending on the context, reaching up to 26.7% in abdominal surgery.4,6–9
Risk factors include preoperative elements (comorbidities, such as obesity and diabetes), intraoperative factors (duration of intervention, type of surgery), and postoperative factors (wound care).10–14 Studies also highlight the impact of practices such as blood transfusions or the surgeon’s experience.10,12,14 Despite preventive strategies recommended by the World Health Organization (WHO; hand hygiene, targeted antibiotic therapy)15 and the CDC (skin antisepsis, glycemic control),16 SSIs remain a major cause of health care-associated infections (20%–30% of cases),17 particularly in resource-limited settings.
Although these risks are documented, few recent studies integrate the challenges of resource-limited contexts, such as that of HEAL Africa hospital (a tertiary care facility in Goma, Democratic Republic of Congo), which faces unique infrastructural and socioeconomic constraints. This prospective study aims to identify the risk factors for SSIs after abdominal surgery in this specific setting and to develop a tailored predictive model, combining clinical data and local prevention practices. By aligning protocols with on-the-ground realities, this research offers avenues to reduce SSIs and improve patient outcomes in similar environments.6,8,18
Materials and Methods
Study type, site, and period
This was a prospective, longitudinal, and analytical study conducted in the general surgery department of HEAL Africa tertiary hospital in Goma, Democratic Republic of Congo. It spanned a period of 1 year from April 1, 2023 to April 1, 2024.
Study population
This study included all patients who underwent scheduled or emergency abdominal surgery during the study period.
Surgical procedures were categorized into 3 groups based on the surgical approach:
-
Abdominal wall surgery: Procedures such as hernia repair (open sutured or mesh-based),
-
Mini-laparotomy: Procedures performed through a small, targeted incision (typically 4–8 cm) using a muscle-splitting technique to access a specific organ, such as appendectomy (via Gridiron, McBurney, or Lanz incision), gastrostomy tube insertion, or stoma formation and closure,19,20 and
-
Laparotomy: Procedures requiring a larger, exploratory incision (eg, midline, paramedian) for extensive intra-abdominal-abdominal operations such as bowel resection, trauma exploration, or peritonitis management.
Patients were followed from the time of their admission until 30 days after the operation. The follow-up included ward round in the hospital department during the admission and outpatient consultation or at the dressing clinic, or by telephone interview after discharge. Followed patient were then postoperatively stratified into 2 groups: those who developed SSIs and those who did not.
Any patient who did not meet the inclusion criteria was not included in this study. Exclusion criteria were as follows:
-
Patients transferred to another facility before completing the 30-day postoperative follow-up period,
-
Patients who were lost to follow-up (ie, not reachable via telephone for postdischarge assessment), and
-
Patients who died intraoperatively, as the outcome of interest (SSI) could not occur.
Our sample was a nonprobabilistic exhaustive sample including all hospitalized patients who underwent abdominal surgery during the study period.
Study variables and data collection
Dependent variable
- Occurrence of a SSI: Defined according to CDC/National Health Care Safety Network criteria5,9 as an infection occurring within 30 days postoperatively (or 1 year in case of an implant), classified into 3 types: superficial (skin/subcutaneous tissue), deep (fascia/muscle), or organ/space (organs or opened cavities).8,21
Independent variables
-
Explanatory variables were grouped into 5 categories:
-
Demographic data: age (<20 years, 20–39 years, ≥40 years), sex (male/female), residence (Goma/outside Goma),
-
Medical/surgical history: Diabetes mellitus, hypertension, malnutrition (assessed by body mass index determination), cancerous pathology, history of laparotomy (yes/no),
-
Preoperative parameters: Preoperative duration (days), wound class (clean/clean contaminated vs contaminated/dirty),5,9 antibiotic prophylaxis (yes/no),
-
Intraoperative parameters: American Society of Anesthesiologists (ASA) score, type of anesthesia (locoregional/general), type of surgery (scheduled/emergency), procedure (classified as mini-laparotomy, full laparotomy, abdominal wall surgery), operative duration (hours), operator qualification (specialist/Surgical resident), and
-
Postoperative parameters: Infectious/noninfectious complications, length of hospital stay (days), survival/death.
-
Data collection
-
Prospective design: Longitudinal follow-up of the 218 patients for 30 postoperative days, including:
-
Hospitalization: Daily nursing wound monitoring was performed. Formal surgical inspection for SSI was conducted on postoperative day 3 and then every 3 days thereafter,
-
Outpatient consultations: Follow-up of dressings and SSI diagnosis in the clinic, and
-
Mobile phone: Calls to patients lost to follow-up to detect late SSIs.
-
-
Sources: Medical records, operative reports, laboratory results (bacterial cultures),
-
Antibiotic therapy: Adaptation of protocols according to wound class8:
-
Clean wounds: Short-course antibiotic therapy (<24 hours),
-
Contaminated/dirty wounds: Prolonged up to 5–7 days for contaminated and ≥7 for dirty following the local policy.
-
Patient preparation and follow-up
Preoperative preparation followed WHO recommendations. For scheduled surgeries, patients received a preoperative shower the night before surgery and the morning of the surgery, and hair removal from incision sites (abdomen/groin) was performed using an electric razor immediately before the surgical procedure. Skin preparation used povidone-iodine and surgeons disinfected their hands by washing with soap followed by hydroalcoholic friction. Ceftriaxone antibiotic prophylaxis was administered intravenously 30 minutes before incision, with adapted doses (2 g for adults, 50 mg/kg for children).
After the intervention, patients were hospitalized and monitored according to a structured protocol. The first wound inspection took place on the third postoperative day (day 3), followed by sterile dressing changes every 3 days until healing. In case of suspected SSI, the responsible surgeon confirmed the diagnosis according to CDC criteria (ie, confirmed by bacteriological analysis: pus collection by sterile aspiration for superficial suppurations or swabbing for cases without visible discharge). Patients were followed for 30 days, including outpatient consultations and telephone interviews for those discharged early. This approach allowed participants to be classified into 2 groups: with SSI (n = 71) and without SSI (n = 147), facilitating comparative analyses.
Microbiological samples were processed according to standardized protocols. Pus or swab samples were transported to the laboratory within 10 minutes, then gram-stained and cultured on aerobic (blood agar) and anaerobic (cooked broth) media. An antibiogram was performed in case of bacterial growth. Negative cultures on day 3 were maintained for up to 8 days to exclude delayed growth. These methods, aligned with WHO and CDC guidelines, ensured accurate identification of pathogens and their resistance profiles.
Statistical analysis
Continuous data, depending on their distribution, were summarized by mean ± standard deviation (normal distribution) or median with interquartile range (non-normal distribution). Categorical variables were described by counts (n) and percentages (%). Comparisons between groups used Fisher’s exact test (expected counts <5) or Pearson’s χ2 test (expected counts ≥5).
Identification of SSI risk factors was based on univariate logistic regression analysis, followed by a multivariate model including significant (P < .05) or clinically relevant variables, selected by forward selection. The discriminatory performance of the final model was assessed using the C statistic (area under the receiver operating characteristic curve).
The significance level was set at P < .05. Analyses were performed using STATA 16.0 (StataCorp LP, College Station, TX).
Ethical considerations
The study was approved by the Medical Ethics committee of the University of Goma (approval number: UNIGOM/CEM/08/2023). Participant anonymity and data confidentiality were strictly preserved. Written informed consent was obtained from each patient before their inclusion in the study.
For patients undergoing elective surgery and for those who were clinically stable upon admission, written informed consent was obtained preoperatively. This occurred after the surgical procedure had been explained but before the patient was taken to the operating theater. For minors and incapacitated adults, consent was provided by a parent or legal guardian.
For patients requiring immediate, life-saving emergency surgery, particularly those operated on during night hours, the urgent clinical need took precedence. In these cases, the process of obtaining informed consent for study participation was deferred to the postoperative period. Consent was sought from the patient (or from a parent or guardian if the patient was a minor, unconscious, or otherwise incapacitated) as soon as their clinical condition was stable. This was typically during the first formal postoperative round on the morning following the surgery.
During this consent discussion, the study’s purpose, procedures, potential risks and benefits, and the strict confidentiality of all data were explained in detail in the patient’s preferred language. It was emphatically stated that participation was entirely voluntary and that the decision to participate or decline would in no way affect the standard of medical or surgical care received. All participants (or their guardians) provided written informed consent. No patients or their representatives opted out of the study. Patients who did not provide consent received the full standard of care but were excluded from data collection and analysis.
Results
Among the 218 patients included (mean age: 27.1 ± 20.3 years; median: 25 years [interquartile range: 8–41]), a majority were male (65.1%, n = 142) and resided in Goma (82.1%, n = 179). Comorbidities included malnutrition (10.6%, n = 23), history of laparotomy (8.7%, n = 19), and cancerous pathologies (4.1%, n = 9). Surgery was performed within 7 days of admission for 79.8% of cases (n = 174), with wounds mostly classified as clean (75.2%, n = 164) and antibiotic prophylaxis administered in 92.7% of cases (n = 202). Most patients were classified as ASA I (79.8%, n = 174), and 52.3% of interventions were scheduled (n = 114), primarily laparotomies (45.9%, n = 100) and hernia repairs (36.7%, n = 80). The median operative duration was 60 minutes [interquartile range: 45–90], with 61.0% of procedures ≤1 hour (n = 133). SSIs occurred in 32.6% of patients (n = 71), associated with a median hospital stay of 7 days.
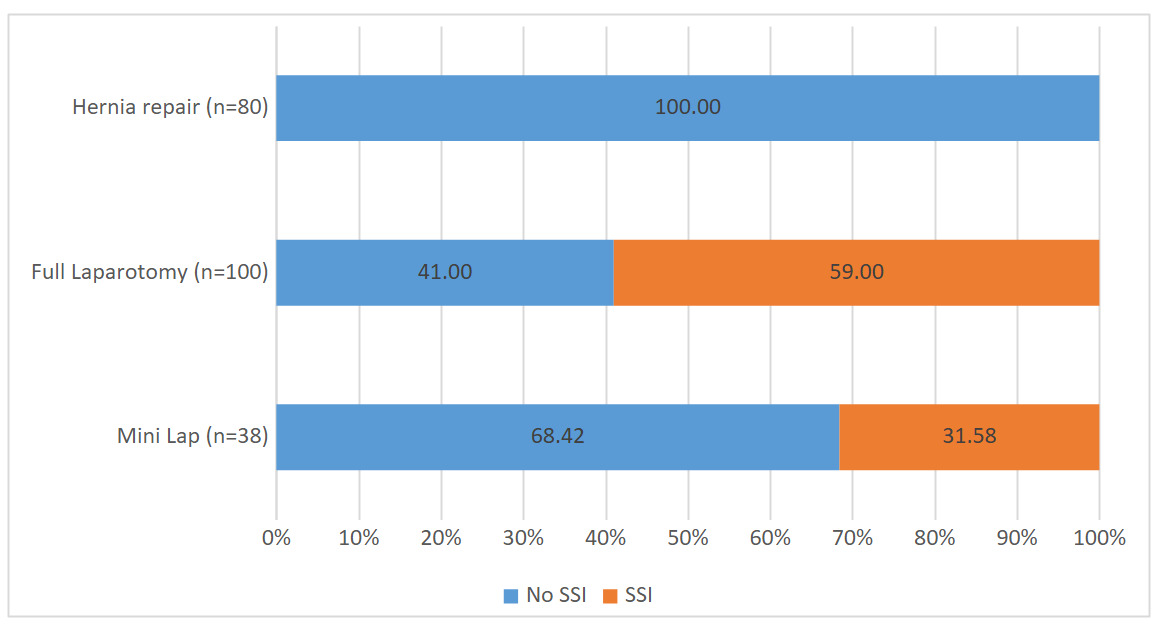
SSI distribution varied significantly by type of surgery (Figure 1): 59% after laparotomy (vs. 0% for hernia repairs, P < .0001) and 31.6% after mini-laparotomy.

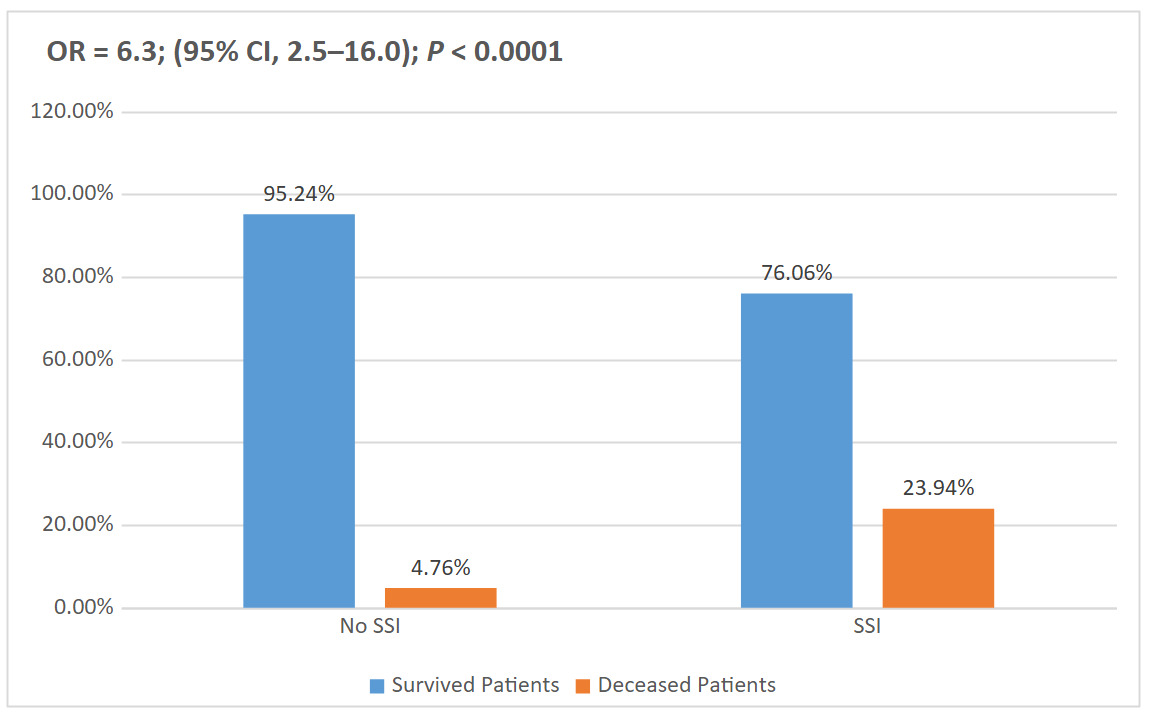
Of the 218 patients, 194 (89.0%) survived and 24 (11.0%) died. A marked disparity was observed between the groups without SSI (survival: 95.24%) and with SSI (survival: 76.06%; death: 23.94%). The analysis reveals a significant association between SSIs and postoperative mortality (odds ratio [OR] = 6.3; 95% confidence interval [CI], 2.5–16.0; P < .0001), as illustrated in Figure 2.

Bivariate analysis identified several factors significantly associated with SSIs. Patient-related factors included age (P = .0024), malnutrition (P < .0001), history of laparotomy (P = 0.006), and cancerous pathologies (P = .026). Procedural factors included a preoperative duration ≥7 days (P < .0001), contaminated wounds (P < .0001), absence of antibiotic prophylaxis (P = .0005), emergency surgeries (P < .0001), laparotomies (P < .0001), and operative duration >1 hour (P < .0001). Conversely, sex (P = .081), ASA classification (P = .105), residence (P = .498), and type of practitioner (P = .055) did not show a significant association (Table 1).
Multivariate analysis identified 4 independent risk factors for SSIs. Laparotomy was associated with a 4.2-fold increased risk (adjusted OR = 4.2; 95% CI, 1.7–10.3; P < .0001), and malnutrition increased this risk by 5.2 times (adjusted OR = 5.2; 95% CI, 1.3–20.7; P = .02). Furthermore, contaminated or dirty wounds (adjusted OR = 4.5; 95% CI, 1.8–11.5; P < .0001) and operative duration exceeding 1 hour (adjusted OR = 15.3; 95% CI, 6.4–36.6; P < .0001) emerged as major predictors, the latter being the factor most strongly associated with SSIs (Table 2).
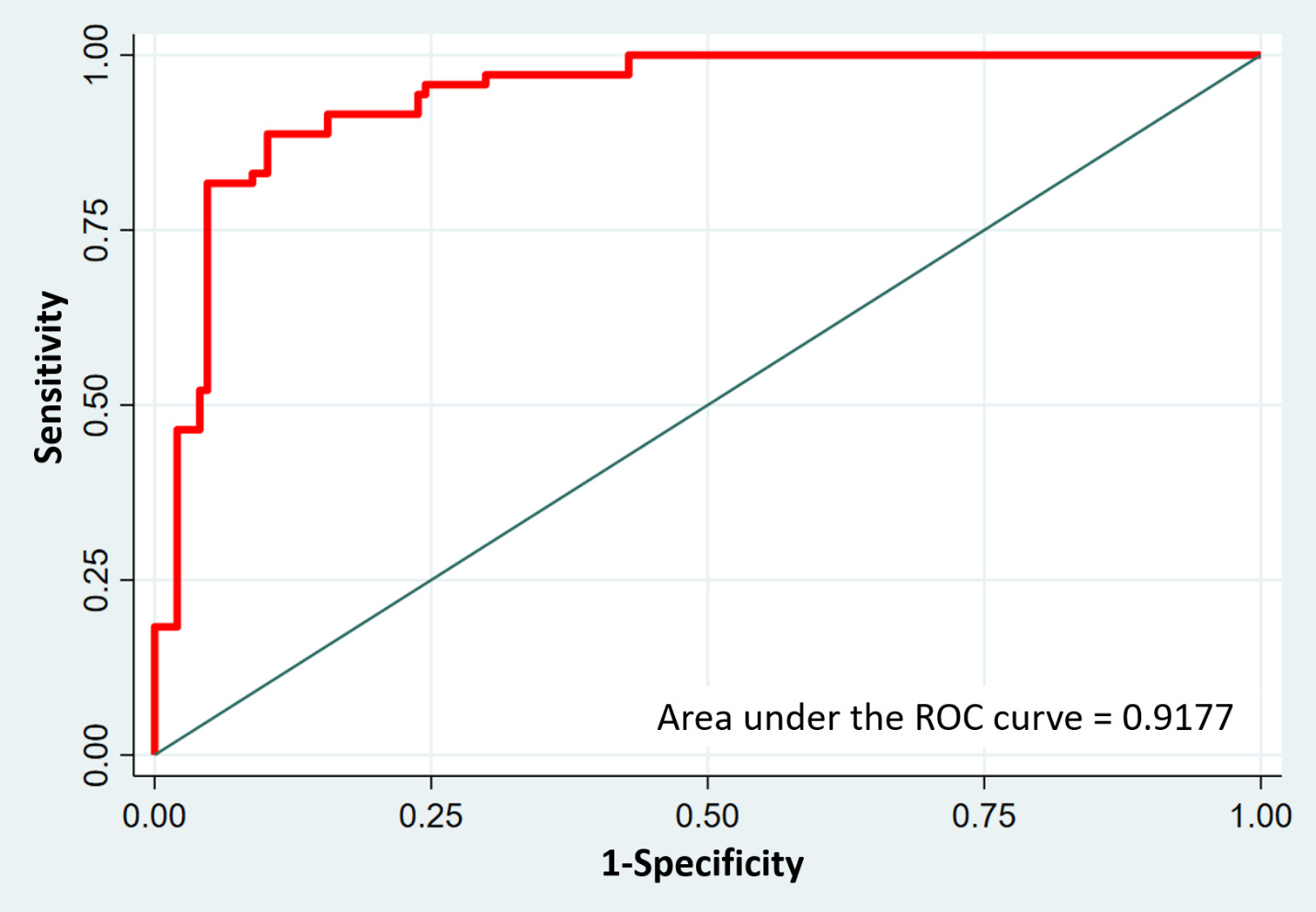
The logistic regression model showed excellent discriminatory performance for predicting SSIs in abdominal surgery, with an area under the receiver operating characteristic curve (area under the curve) of 0.917 (95% CI, 0.876–0.958; P < .001), indicating high predictive accuracy (Figure 3).

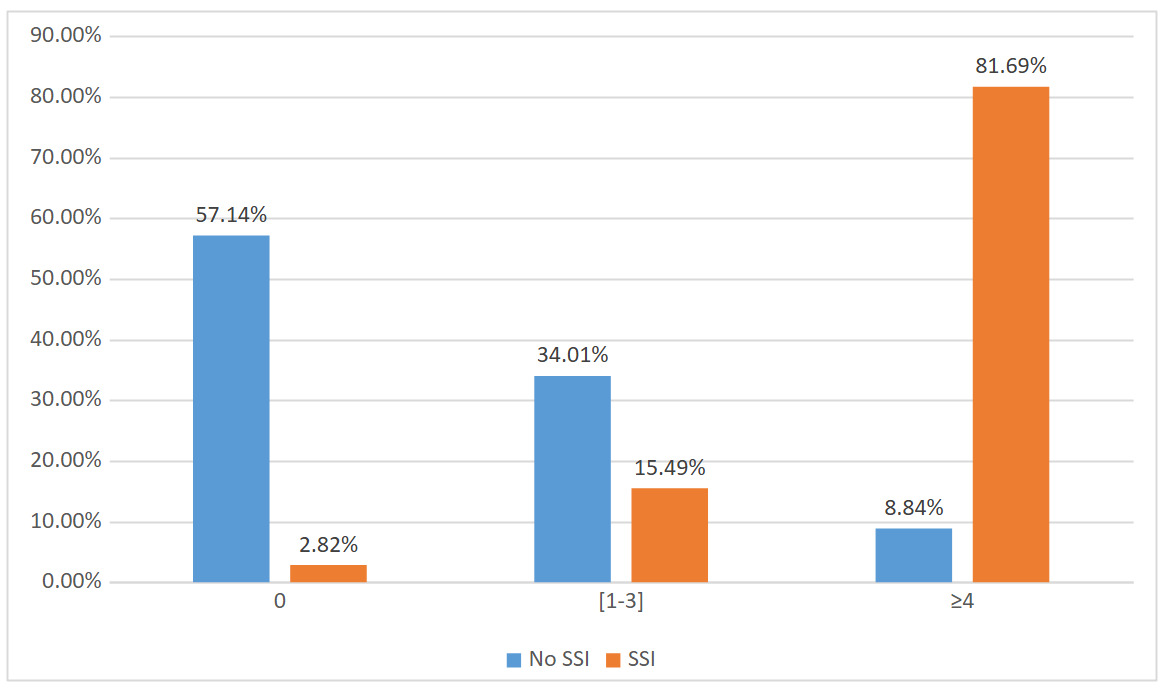
The average SSI risk score was 2.3 ± 2.4 for all patients. A significant difference was observed between the groups with SSI (4.8 ± 1.8) and without SSI (1.1 ± 1.6, P < .0001). Analysis stratified by score thresholds (0, 1–3, ≥4) revealed a gradual increase in SSI incidence with increasing score (Figure 4). These results confirm the predictive value of the score for identifying high-risk patients, offering a potential tool for optimizing preventive strategies in clinical practice.

Discussion
Our study revealed an SSI incidence of 32.6% in patients undergoing abdominal surgery at HEAL Africa hospital. The incidence of SSIs observed in our study stands notably higher than figures reported in comparable research. When we examined the broader literature, we found Aga et al7 documented SSIs in 22.2% of abdominal surgery cases in their prospective study. Alkaaki et al9 reported a slightly lower rate of 16.3%, whereas data from Guzmán-García et al8 from a Mexican cohort showed just 12% incidence. Interestingly, Hernandez et al6 findings from a Peruvian hospital came closest to our results at 26.7%. This variation across studies reflects profound differences in clinical environments and patient populations. At HEAL Africa hospital in Goma, we’re confronting challenges that many better-resourced settings don’t face to the same degree. Our patients often present with advanced disease due to delayed presentation, and our surgical teams work with constrained resources. The socioeconomic realities of our region, where malnutrition is endemic and access to basic medical care remains inconsistent, create a perfect storm for postoperative complications. These contextual factors explain much of the disparity between our SSI rates and those reported elsewhere.
When we examined the specific risk factors contributing to SSIs, malnutrition emerges as particularly devastating. Our adjusted odds ratio of 5.2 (95% CI, 1.3–20.7; P = 0.02) confirms what surgeons have long suspected: a malnourished patient faces dramatically worse surgical outcomes. This finding aligns with Pessaux et al16 earlier work and makes physiological sense when we consider how hypoalbuminemia, which is marker of chronic malnutrition, impairs the wound healing and immune function. The work of Guzmán-García et al8 and Haridas and Malangoni17 has well elucidated this mechanism, showing how depleted protein stores leave patients vulnerable to infection at precisely the moment they need robust defenses.18,21 In our clinical experience, these patients don’t just develop infections more often, their infections tend to be more severe, more persistent, and more likely to require reoperation. The downstream consequences include prolonged hospital stays that strain limited bed capacity,22,23 high treatment costs that families can ill afford,24,25 and in some cases, entirely preventable deaths. This is why we’ve begun implementing mandatory nutritional screening for all elective abdominal surgery cases.
The choice of surgical approach plays an equally critical role in infection risk. Our data reveal that laparotomy carries a 4.2-fold higher SSI risk compared to abdominal wall procedures like hernia repairs or mini-laparotomy approaches such as appendectomy (adjusted OR = 4.2; 95% CI, 1.7–10.3; P < .0001). We suspect this risk differential would be even more pronounced if we could compare it to laparoscopic techniques, though our current setting doesn’t yet permit such minimally invasive approaches. This can be explained by the fact that a large midline incision represents a massive insult to the abdominal wall’s integrity and this creates an extended portal for microbial invasion and simultaneously compromises local tissue perfusion. Ming et al’s12 work on laparoscopic appendectomy demonstrates the flip side of this equation, showing how smaller incisions translate directly to fewer infections. Yet in our setting, laparotomy remains necessary for many cases due to both the advanced pathology we encounter and our limited access to advanced laparoscopic equipment. The patients who most often require these open approaches—those with complex comorbidities like uncontrolled diabetes or morbid obesity—are precisely those least equipped to fight off subsequent infections.26,27 It’s a cruel paradox that demands constant vigilance in our preoperative planning and postoperative monitoring.
Operative duration emerged as our most striking risk factor, with procedures exceeding 1 hour showing a staggering 15.3-fold increase in SSI risk (adjusted OR = 15.3; 95% CI, 6.4–36.6; P < .0001). The CI here leave little room for doubt about the magnitude of this effect. This finding, consistent with numerous previous studies,4,6,8,9,16,28 reflects multiple compounding hazards. Every additional minute under anesthesia represents another opportunity for bacterial colonization, another increment of immunosuppression from surgical stress, and another decline in tissue antibiotic concentrations.29 The physical reality of prolonged retraction and manipulation causes measurable tissue trauma that becomes increasingly difficult for the body to repair. In our resource-constrained hospital setting, where we routinely manage complex surgical cases, we face constant tension between surgical completeness and operative efficiency. These clinical dilemmas become most acute when deciding to weigh the infection risks of prolonging a difficult procedure against those of accepting a less-than-ideal repair.
The classification of surgical wounds was a key factor in predicting infection risk. Our analysis revealed that contaminated or dirty wounds carried a 4.5-fold higher risk of SSI compared to clean and clean contaminated wounds (adjusted OR = 4.5; 95% CI, 1.8–11.5; P < 0.0001). This finding aligns with extensive clinical evidence,4,6,7,9,14,30–32 confirming what surgeons encounter daily: wounds exposed to heavy bacterial loads create an ideal environment for infection. When microorganisms penetrate deep tissues,15,33 they don’t just slow healing, they trigger a cascade of complications, leaving patients vulnerable to persistent infections.9,15,16
The problem extends beyond local wound issues. Contaminated tissues provoke an intense inflammatory response that can spiral into systemic infection, turning a manageable postoperative course into a life-threatening scenario. This is why we’ve learned that meticulous infection control isn’t just beneficial, it’s nonnegotiable. From strict adherence to sterile technique to timely antibiotic administration, every precaution matters. But our responsibility doesn’t end in the operating room. Close postoperative surveillance, identifying early signs of infection, and intervening before complications escalate can make the difference between a routine recovery and a prolonged hospital stay.
In abdominal surgery, where wound contamination often reflects the underlying pathology, proactive management isn’t just a best practice, it’s a critical safeguard for patient outcomes.
Although this prospective study provides valuable insights into SSI risk factors, several limitations warrant consideration. Most notably, we were unable to collect complete data on several known infection predictors, including obesity, diabetes, and smoking status, due to challenges in patient follow-up in our resource-constrained setting. These gaps may affect the precision of our risk estimates and limit direct comparisons with studies from better-equipped facilities.
The heterogeneous nature of our surgical population, encompassing everything from elective hernia repairs to emergency laparotomies, also presents interpretive challenges. Although this diversity reflects real-world practice at HEAL Africa hospital, it means our findings may not apply equally to all abdominal procedures. We also recognize that unmeasured social determinants, like nutritional access, home sanitation, and transportation barriers to follow-up, likely influence outcomes in ways our clinical data couldn’t capture.
Yet these limitations don’t diminish the study’s value. Rather, they highlight the complex realities of surgical care in low-resource environments. Our findings provide a crucial foundation for quality improvement initiatives and underscores the need for enhanced data collection systems to better address these knowledge gaps in future research.
In addition, the study has significant strengths. With a sample of 218 patients, it allows for robust statistical analysis. The use of multivariate regression models strengthens the validity of the conclusions by accounting for confounding variables. By focusing on a specific population at HEAL Africa hospital in Goma, it provides relevant information for improving local practices. The rigorous classification of SSIs according to CDC definitions ensures the comparability of results with other studies. The study also identified important risk factors, such as the type of operation, malnutrition, wound class, and operative duration, which are useful for developing prevention strategies.
Conclusion
This study highlights a high incidence of SSIs after abdominal surgery at HEAL Africa hospital (32.6%), with a significantly higher mortality rate in patients with SSIs (23.94%) compared to those without SSIs (4.76%). Independent risk factors identified include laparotomy, malnutrition, contaminated or dirty wounds, and operative duration exceeding 1 hour, the latter being the most powerful predictor (adjusted OR = 15.3). The predictive model developed shows remarkable discriminatory performance (area under the curve = 0.917), validated by a stratified risk score showing a gradual increase in SSI incidence with increasing score. These results emphasize the need for targeted preventive strategies, including preoperative optimization of nutritional status, reduction of surgical delays, and adoption of reinforced antisepsis protocols, particularly in resource-limited contexts like Goma. Integrating the risk score into clinical practice could improve early identification of high-risk patients and guide personalized interventions, thereby reducing morbidity, associated costs, and postoperative mortality in similar environments.
Ethical Approval
The study was approved by the University of Goma’s Medical Ethics Committee (UNIGOM/CEM/08/2023).
Informed Consent
Written, informed consent was obtained from all participants.
Data Availability
The datasets generated and analyzed during the current study are not publicly available due to patient confidentiality agreements but are available from the corresponding author upon reasonable request.
Conflict of Interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.