Introduction
Traumatic injuries remain one of the leading global health issues, causing more than 5 million deaths annually worldwide and this burden exceeds the combined burdens of HIV, malaria, tuberculosis, and COVID-19.1 Furthermore, traumatic injuries disproportionately affect low- and middle-income countries (LMICs), where more than 90% of injury-related deaths occur. Road traffic accidents (RTAs) account for the majority of these fatalities and primarily impact young adults, leading to long-term disability, loss of productivity, and socioeconomic consequences.1
In Uganda, traumatic injuries rank among the 7 leading causes of mortality, accounting for approximately 5.95% of injury-related deaths in 2021 and RTAs account for 33.3% of all injury-related deaths, equivalent to an incidence rate of approximately 15.07 deaths per 100,000 people.2,3 The recent police data revealed a 16% increase in the incidence rate of RTAs between 2022 and 2023; moreover, this increase was nearly 40% among motorcycle-related RTAs.3 Many of these deaths can be prevented through timely prehospital interventions, especially basic on-scene care such as hemorrhage control and rapid transport.
The World Health Organization recommends the establishment of lay first responder (LFR) programs as an initial step toward strengthening emergency care systems in settings with limited formal prehospital services.4 Such programs train non-health professionals e.g., police officers, motorcycle riders, taxi drivers, and community leaders; to provide essential life-saving care at injury sites and during transport.
Herein, we examine LFR training as a pragmatic and equity-oriented approach to strengthening prehospital trauma care in Uganda. Evidence was drawn from regional and global literature, which was retrieved via through targeted searches of PubMed, African Journals Online (AJOL), and Google Scholar by using key terms such as “lay first responders,” “prehospital trauma care,” “first aid training,” “road traffic injuries,” “emergency medical services,” and “Uganda.” Additionally, we reviewed relevant grey literature, including reports and policy documents from the World Health Organization, the Uganda Ministry of Health, the Uganda Police Force, and implementing partners. Furthermore, the authors’ practical experiences were considered. These sources were synthesized to assess the feasibility, knowledge and skills acquisition, and cost-effectiveness of training non-health professionals as well as to propose context-specific strategies for nationwide scaling.
State of Prehospital Emergency Care and Lay First Responder Programs in Uganda
Uganda has made notable progress toward formalizing emergency medical services (EMS) through the establishment of a national EMS Committee and development of the National EMS Policy, Guidelines, and Strategic Plan (2019/20–2024/25). The key objectives of this plan include expanding access to on-scene emergency care and improving ambulance response times nationwide.5 However, the implementation of this plan remains uneven, and access to timely prehospital care remains limited outside of urban and peri-urban centers.
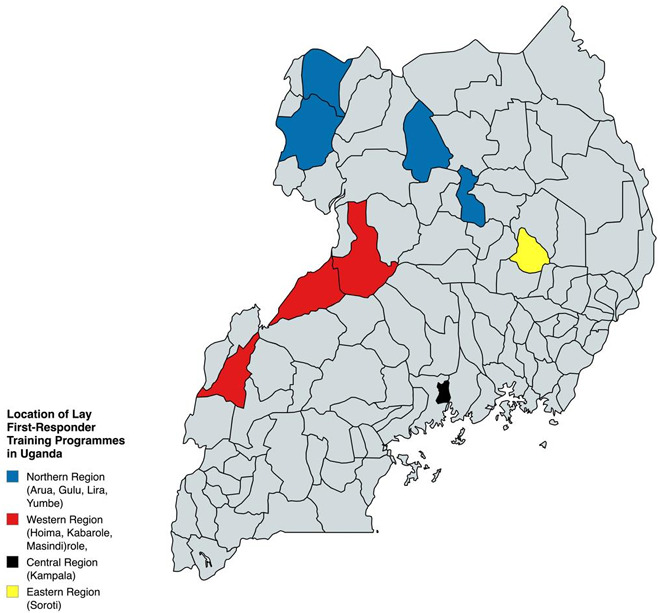
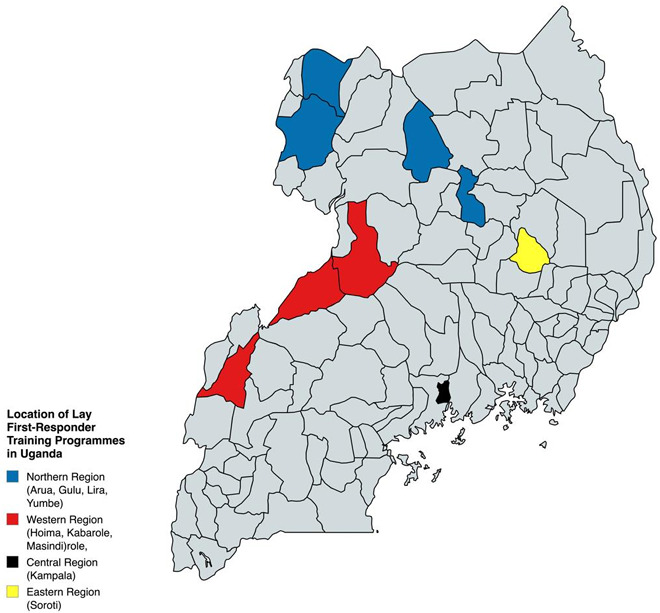
Although formal EMS development has been prioritized, LFRs remain underutilized. In many settings, bystanders are the first people to reach injury scenes and could provide essential life-saving interventions if they were adequately trained and equipped. In Uganda, the existing LFR programs are largely concentrated in Kampala and a few peri-urban areas, leaving significant geographic deserts (Figure 1). While national data directly linking LFR coverage to mortality outcomes are limited, the available evidence suggests that early on-scene interventions are critical determinants of survival after traumatic accidents in resource-constrained settings.
Why Prioritize a Nationwide Lay First Responder Program?
Traumatic injuries impose substantial health and socioeconomic burdens in Uganda, disproportionately affecting working-age adults and exacerbating poverty through disability, prolonged hospital stays, and lost income.1,2,6 Therefore, injury prevention and early care are not only health priorities but also matters of social justice and national development. It is essential for the materialization of universal health coverage as well as Uganda Vision 2040, which envisions “A Transformed Ugandan Society from a Peasant to a Modern and Prosperous Country within 30 years.”7
LFR training represents a feasible and cost-effective complement to the development of a formal EMS framework.8,9 Evidence from Uganda and comparable LMICs demonstrates that non-health professionals can acquire and retain essential trauma care knowledge and skills, including hemorrhage control and safe patient transport.9 While there is little direct evidence regarding the effect of LFR training on population-level mortality reduction, studies consistently show improved early care processes and favorable cost-effectiveness. For example, Jayaraman and colleagues demonstrated that it would cost less than $100 per life-year saved to scale up an LFR program in Kampala.8 Additional studies suggest that LFR programs are substantially more affordable in the short to medium term than comprehensive EMS expansion, thus making these programs a pragmatic first step for strengthening prehospital trauma care.9,10
The Future of Lay First Responder Programs in Uganda: Implementation Considerations
Scaling up LFR programs at the national level will require coordinated, multisectoral engagement. Some key stakeholders include the Ministry of Health, the Uganda Police Force, the Uganda National Road Authority, transportation associations, local governments, civil society organizations, the Uganda Red Cross Society, and other nongovernmental organizations (NGO) involved in injury prevention and health care. Embedding first aid and trauma response training within driver/rider licensing and transport sector regulation offers a sustainable pathway for scaling these programs, while mandatory refresher courses can maintain skill retention.
Sustainable financing remains a critical barrier to the implementation of LFR programs. Potential robust financing mechanisms include integration into national road safety budgets, public–private partnerships with transport and telecommunications companies, and corporate social responsibility initiatives. Alignment with Uganda’s EMS Strategic Plan is essential to ensure that LFR programs complement rather than replace formal EMS frameworks.
Robust monitoring and evaluation frameworks are needed to guide the implementation and assess the impact of LFR programs. Establishing a national trauma registry would enable the systematic tracking of prehospital interventions, patient outcomes, and regional disparities, thereby informing continuous system improvement and future research on effectiveness and sustainability.
Conclusion
Nationwide scale up of LFR programs represents a practical and equity-oriented strategy for improving on-scene trauma care in Uganda. While LFR programs are not a replacement for formal EMS systems, they are an essential foundation for strengthening prehospital care in resource-constrained settings. By embedding these programs within national policy frameworks, driver/rider licensing processes, and sustainable financing mechanisms, Uganda can reduce preventable trauma deaths and advance progress toward both universal health coverage and Vision 2040. Continued investment in monitoring, evaluation, and research will be critical to ensure long-term effectiveness and system integration.
Acknowledgments
We wish to acknowledge the ministry of health, Uganda, and all individuals and organizations working to promote equitable access to timely and appropriate pre-hospital care for injury victims.
Ethical Approval
There was no ethical approval required for this study
Informed Consent
Not required
Data Availability
No data to be made available
Conflict of Interest
Authors have no conflict to disclose
Funding
No funding was received for this work