Introduction
Infantile hypertrophic pyloric stenosis (IHPS) is a leading surgical cause of nonbilious vomiting in early infancy and results from progressive hypertrophy of the pyloric circular muscle, ultimately causing gastric outlet obstruction.1–3 Although well-recognized clinically, the underlying etiology remains incompletely understood.
Globally, the incidence of IHPS ranges from 1.5 to 4 per 1000 live births, with notable variation across geographic and ethnic groups. The condition exhibits a pronounced male predominance, with a male-to-female ratio of 4:1 to 6:1. Multiple risk factors have been proposed—including genetic susceptibility, bottle feeding, maternal smoking, and macrolide exposure—yet these associations differ across populations, and no single causal mechanism has been definitively established.4–6
In Africa, literature on IHPS remains relatively limited, but available studies from Nigeria, Cameroon, and Ethiopia report comparable clinical patterns to those in high-income settings. However, variations in age at presentation, nutritional status, and perioperative outcomes are frequently observed. Ethiopia, in particular, delayed presentation and diagnosis have been consistently noted, contributing to higher rates of dehydration, electrolyte disturbances, and malnutrition by the time of surgical intervention.7–9
Clinically, infants with IHPS usually present between the ages of 3 and 5 weeks with progressive, projectile, nonbilious vomiting. If unrecognized, prolonged vomiting can lead to severe dehydration, metabolic alkalosis, electrolyte derangements, and significant malnutrition, all of which may complicate perioperative management and recovery.5–10 Despite these risks, Ramstedt’s pyloromyotomy remains the gold-standard treatment worldwide, with outcomes heavily influenced by timely diagnosis, adequate preoperative resuscitation, and optimal postoperative care.10–21
Given the contextual differences in presentation and perioperative challenges in low- and middle-income countries, understanding local patterns is essential for improving outcomes. Therefore, this study aims to assess the clinical profile and surgical outcomes of infants diagnosed with IHPS at Hawassa University Comprehensive Specialized Hospital (HUCSH). By examining demographic characteristics, clinical manifestations, radiologic and laboratory findings, and perioperative and postoperative factors, the study seeks to identify key determinants of outcomes and highlight areas for strengthening care in similar resource-limited settings.
Methodology
This study was conducted at HUCSH, located at 7°3’N and 38°28’E on the eastern shore of Lake Hawassa, Sidama. HUCSH is a major teaching and referral center serving an estimated 20 million people from the Sidama Region, SNNPR, southern Oromia, the Somali Region, as well as parts of Somalia and Kenya. Established in 2003, the hospital has approximately 450 beds and delivers clinical and emergency services to more than 102,000 patients annually. A dedicated pediatric surgery unit was initiated in 2017 with one pediatric surgeon and has since expanded to 3 pediatric surgeons, enhancing clinical care, postgraduate training, and pediatric surgery research capacity.
A retrospective cohort study was conducted from January 2018 to December 2024 to evaluate the relationship between preoperative risk factors and postoperative outcomes in infants diagnosed with IHPS. A cohort design was selected to establish temporal associations between exposures and outcomes using existing medical records, which would not be adequately addressed through a cross-sectional approach. All medical records of infants diagnosed with IHPS during the study period constituted the source population. Records were included if they contained complete information for all major study variables, while charts with incomplete essential data were excluded.
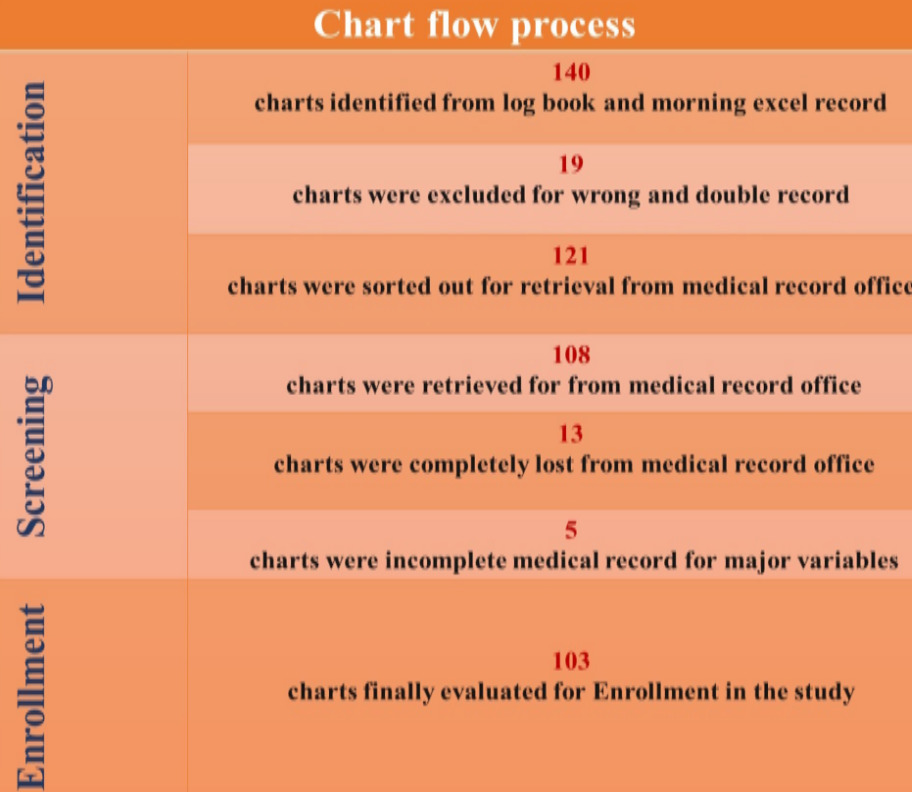
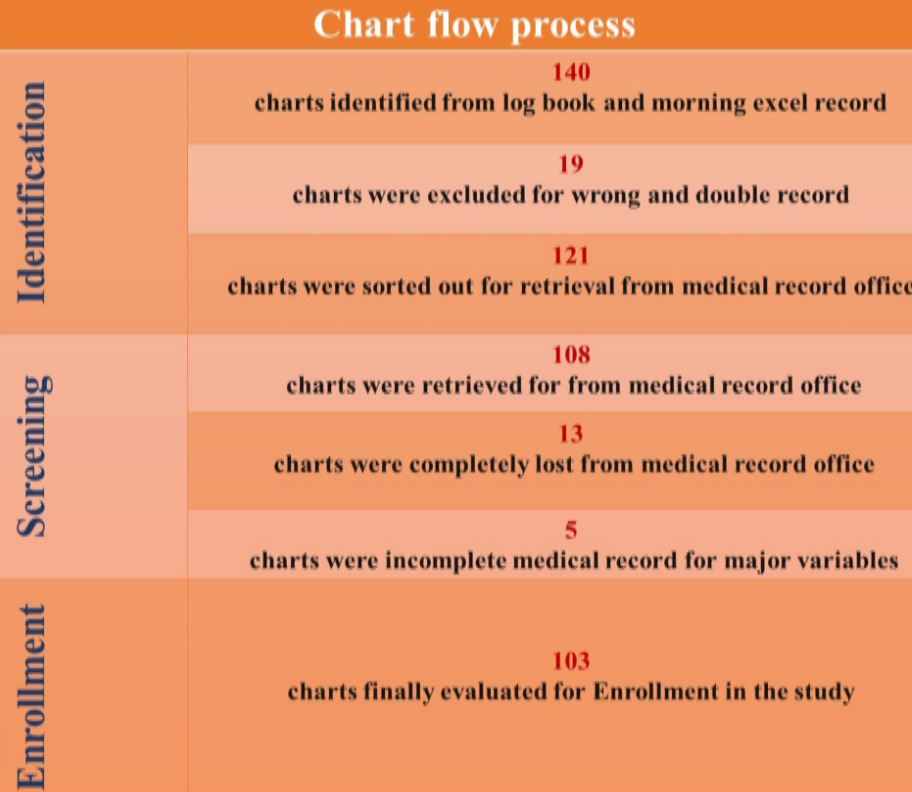
A census approach was applied to maximize case capture, whereby all eligible IHPS cases were reviewed. During the study period, 121 infants underwent Ramstedt’s pyloromyotomy, and 103 were included based on data completeness and eligibility (Figure 1). Data were collected after obtaining IRB approval by trained nurses, medical interns, and junior surgical residents using a structured checklist. Medical record numbers were identified from daily departmental reports, pediatric emergency and pediatric surgery ward logbooks, and operation theatre registries. Extracted data were entered into the Kobo Toolbox system.
To ensure data quality, the checklist was pretested, each record was assigned a unique code, and the final dataset was exported to SPSS version 26.3 for analysis. Descriptive statistics were generated, followed by bivariable and multivariable binary logistic regression analysis to identify independent factors associated with surgical outcomes. Study variables included demographic characteristics (age, sex, birth order), clinical and nutritional status (admission weight, severity of malnutrition, duration of symptoms, degree of dehydration, electrolyte disturbances), intraoperative events (mucosal perforation), postoperative complications (surgical site infection, wound dehiscence, reoperation), and hospital stay. The primary outcome was defined as long-term surgical success, measured by absence of reoperation and major complications, while secondary outcomes included postoperative complications, feeding outcomes, duration of hospitalization, trends, and potential risk factors influencing surgical results.
Operational definitions
Delayed Presentation: Infants presenting to the hospital > 3 weeks after symptom onset (vomiting, feeding intolerance, poor weight gain).
Severe Malnutrition: Weight-for-length Z-score <-3 SD (WHO criteria) as of all admitted patients had record of complete anthropometric data up on chart evaluation and screening
Prolonged Hospital Stay: Postoperative stay > 5 days after pyloromyotomy, exceeding the expected 2–3 days.
Perioperative favourable surgical outcome; No major complications or hospital re-admission and anaesthesia related major adverse events identified during treatment and follow ups
Perioperative unfavourable surgical outcome; Any major adverse perioperative event, including complete wound dehiscence, reoperation, persistent vomiting, complicated hospital acquired infections, or severe electrolyte disturbances requiring correction.
Reoperation rate; Any need to repeat surgical intervention required due to incomplete pyloromyotomy, postoperative complications, or other surgery-related issues during the hospital stay.
Postoperative Feeding Protocol; Nongraded (Ad Libitum) Feeding Protocol: Full oral feeding is initiated soon after Ramstedt’s pyloromyotomy, typically 4–6 hours postoperatively, without stepwise increases, unless the infant exhibits intolerance such as vomiting or abdominal distension. This approach was applied to all infants in the study.
Results
In this study for the purpose of analysis and presentation, the study variables were categorized according to standard pediatric surgery textbooks, previously published literature, and relevant World Health Organization (WHO) guidelines. This approach was used to ensure consistency with established clinical definitions and to facilitate meaningful comparison of the study findings with existing evidence.
Sociodemographic characteristics of infantile hypertrophic pyloric stenosis at HUCSH
Male predominance was observed, with 86 (83.5%) of patients’ being male, the majority of infants 41 (39.8%) aged between (3–4) weeks at presentation, while the median age of infants at presentation was 4 weeks (IQR; 3–7). However, we observed one patient presented at the age of 20 weeks. Urban residents accounted for 60 (58.3%), while rural residents were 43 (41.7%). Birth order was first born in 53 (51.5%) and non-first order born (second, third, and fourth) 50 (48.5%) of infants. Maternal age was mostly between 20–30 years 63 (61.4%) while 21 (20.4%) were above 30 years. 93 (90.3%) mothers reported no exposure to erythromycin. Exclusive breastfeeding was the predominant feeding practice (90/103, 87.4%) (Table 1).
Clinical characteristics profile of infantile hypertrophic pyloric stenosis at HUCSH
Duration of symptoms varied: majority 51 (49.6.%) had symptoms for (3–4) weeks while the median duration of symptoms is 3 weeks (IQR; 1–3), with one case presented after 8 weeks of symptoms, Classic IHPS symptoms (projectile, nonbilious vomiting) were present in 88 (85.4%), while atypical presentations were seen in 15 (14.6%). Significant but unquantified weight loss reported in 78 (75.7%), while the median admission weight was 3.40 kg (IQR; 3.0–3.8), fever in 87 (84.5%), and severe dehydration in 87 (84.5%). Severe acute malnutrition was identified in 98 (95.1%) of infants. Palpable abdominal mass was not appreciated on abdominal examination in 93/103 (90.3%) of infants (Table 2).
Radiological and laboratory findings infantile hypertrophic pyloric stenosis at HUCSH
Laboratory and imaging findings were assessed to evaluate the physiological and anatomical characteristics of infants with IHPS at presentation. Electrolyte imbalances and pyloric measurements were analyzed to determine the severity of illness and guide perioperative management. Serum potassium was within the normal range (3.5–5.5 mEq/L) in 75 (72.8%) infants, while 28 (27.2%) exhibited hypokalaemia.
Chloride abnormalities were the most common electrolyte derangement observed in 67 (65%) infants, exhibited variable range of hypochloraemia and hyponatremia observed in 44 (40.8%) of infants. Pyloric muscle thickness exceeded 5 mm in 94 (91.3%) infants, and 44 (42.7%) had a thickness greater than 6 mm. Pyloric channel length was greater than 20 mm in 62 (60.2%) infants (Table 3).
Perioperative characteristics pattern of infantile hypertrophic pyloric stenosis at HUCSH
All patients received prophylactic antibiotics within 30 minutes of induction and were managed under general anaesthesia with endotracheal intubation. Surgery was performed by fourth-year general surgery residents under supervision of consultant in 100 (97.1%) of cases; consultant pediatric surgeons were directly involved in 3 (2.9%). Anaesthesia providers included MSc anaesthetists 77 (74.8%), BSc anaesthetists 24 (23.3%), and fully trained anaesthesiologists 2 (1.9%), and anaesthesia related complications were peri intubation aspiration 3 (2.9%), delayed awakening 4 (3.8%), and post operative apnea 1(0.9%) of all improved and discharged.
All patients underwent open standard Ramstedt’s pyloromyotomy via right upper quadrant transverse incision in 82 (79.6%) and the rest midline omega incision. Intraoperative mucosal perforation occurred in 1(0.9%). Postoperative feeding started as per Ad libitum protocol with breast milk at 4–6 hours. Postoperative complications were surgical site infection 4 (3.8%), incomplete myotomy 2 (1.9%), wound dehiscence 2 (1.9%), hospital acquired pneumonia 3 (2.9%), meningitis 1 (0.9%), and incisional hernia 1(0.9%). Reoperation was required in 5 (4.85%). Majority of infants 74 (71.84%) discharged within 5 days that exceeding expected 2–3 days. Overall, 96 (93.32%) were discharged without major complications (Table 4).
Binary logistic regression analysis of infantile hypertrophic pyloric stenosis at HUCSH
To identify factors influencing surgical outcomes in infants with IHPS, Correlation Chi-square test, Fishers’ exact test and binary logistic regression analysis were performed. Binary logistic regression analysis identified delayed presentation as independent predicting factor of poor surgical outcomes, (AOR = 6.49, 95% CI 6.25–9.96, P = .041), stating infants with delayed presentation were significantly more likely to have unfavourable surgical outcomes compared to those who presented early. Specifically, infants with delayed presentation had 6.49 times odds of unfavourable surgical outcomes. Despite lack of statistical significance severe malnutrition and electrolyte disturbances remain relevant factors, that may increase risk of post operative complications. (Table 5).
Discussion
In this 6-year retrospective cohort, IHPS showed a strong male predominance, with 83% of cases occurring in male infants—consistent with global reports indicating a male-to-female ratio of 4:1 to 6:1.2,3,5,16,18,21,22 Most infants in our cohort study presented for surgery between 3 to 4 weeks of age, while median age of diagnosis was 4 weeks. This is consistent with global data, where the mean age at diagnosis typically falls between 30.8 and 43 days. However, one case was diagnosed at 140 days (20 weeks), attributed to initial misdiagnosis and delayed referral. Similarly, a study from Nigeria reported a mean diagnosis age of 49 days (7 weeks), also linked to delayed referrals.1–3,16,18
Birth order distribution in our study was nearly equal, differing from reports that associate IHPS more commonly with first-borns. The highest proportion of cases was observed among first born children 53 (51.5%), followed by non-first-borns 50 (48.5%), which may reflect population-specific birth order risk patterns comparable with the existing global data.
About 58.3% of infants were from urban areas and 41.7% from rural regions. Despite this, there was no notable difference in the timing of presentation between urban and rural patients. Most mothers were aged 20–30 years, and no association was found between IHPS and extreme maternal age, antenatal erythromycin exposure, or bottle feeding. Exclusive breastfeeding was common (87.4%), may be suggesting cultural norms that influence feeding practices more than risk profiles, in contrast to global data where these factors are considered important.5,16,18,19
Electrolyte abnormalities were a prominent feature in this cohort, with hypochloraemia being the most common, followed by hypokalaemia. These findings align with data from Ethiopia and Nigeria, where late presentation was also linked to hypokalaemia and hyponatremia.. Globally, studies from the United States and the United Kingdom have shown that hypochloraemia and metabolic alkalosis are reliable indicators of prolonged illness and are often associated with extended preoperative stabilization, though not necessarily with worse surgical outcomes. European studies have reported an association between hypokalaemia and increased postoperative mortality. However no statistically significant association observed in our cohort.
Additionally, in our stud no correlation was observed between pyloric muscle thickness and clinical variables such as age, admission weight, and duration of symptoms. No correlation was found between these variables, contrasting with studies from Pakistan and the United States, where stronger associations have been reported between sonographic measurements and the chronicity or severity of illness.16–21
All patients underwent open standard Ramstedt’s extra mucosal pyloromyotomy, the gold-standard procedure first introduced in 1912. Complications were rare, with only one case of mucosal perforation 1 (1.0%), which is lower than reports from Addis Ababa and other centers where mucosal perforation rates ranged from 9.5%–10.9%. even though it’s difficult to have acceptable generalization of such complication difference in similar resource setting, it needs further multicenter and comparative studies for better generalization.22–28
Overall postoperative complications were observed in 7 (6.68%) infants, such as surgical site infections, incomplete myotomy, wound dehiscence, incisional hernia, meningitis and hospital acquired pneumonia. The reoperation rate 5 (4.85%) in our cohort was slightly in the midrange of the global trend of 2–8%, as reported in studies from Switzerland and Pakistan.11,18,19,29
In this study, independent predicting factor associated with unsatisfactory outcomes was delayed presentation, based on adjusted odds ratios from binary logistic regression. Despite lack of statistical significance, severe malnutrition and electrolyte disturbances remained relevant factors that may increase risk of post operative complications. These conditions often result from delayed presentation, reinforcing timely recognition and early referral. These findings also align with some global reports, such as those from Nigeria and Ethiopia, where electrolyte disturbances have been linked to increased mortality, particularly when associated with delayed presentation and prolonged vomiting.3–9,16,23–26,29–31
This 6-year retrospective study provides one of the most comprehensive analyses of IHPS in Ethiopia, delayed presentation as independent predictors of poor outcomes, based on statistical analysis. The study will help the researchers to focus on factors affecting surgical outcomes of IHPS and open more research question, and guide future researchers to make prospective multicenter studies in our setups and similar settings.
Limitations of the Study
This study is subject to some limitations. Data were retrospectively collected from manually recorded patient charts, introducing challenges related to legibility and completeness. Poor handwriting and documentation practices affected the accuracy and reliability of data extraction. A number of patient charts were missing or lost, reducing sample size and. Several important clinical variables—including birth weight, urine output, and postoperative weight gain—were inconsistently recorded or entirely absent. The retrospective nature further limits control over potential confounders and precludes assessment of causal relationships.
Conclusion
This 6-year experience reflects that IHPS can be treated safely in a surgical training hospital setting along with skill transfer and close mentorship of surgical residents. The study provides detailed insight into the local clinical profile of patients’, indicating delayed presentation as an independent predicting factor of poor outcome, despite lack of statistical significance. Severe malnutrition and electrolyte disturbances remain relevant factors that may increase risk of post operative complications. These conditions often result from delayed presentation, reinforcing timely recognition and early referral. These findings may guide strategies to optimize perioperative care and basics for future IHPS research in our setups and similar settings.
Recommendations
Improving IHPS outcomes requires timely diagnosis and referral, correction of fluid and electrolyte imbalances, and attention to factors contributing to unfavourable surgical outcomes. Establishing an electronic medical record system at HUCSH can enhance data quality. Prospective multicenter studies with larger sample sizes are recommended to identify independent predictors of surgical outcomes.
Ethical Approval
The study was conducted after the institution review board approval letter was obtained from Hawassa university college of medicine and health science institutional review board, research ethical committee waving individual consent with registration number of IRB/632/2025. The data was extracted anonymously, and confidentiality was assured at each step of data collection and processing. The study complies with the principles of Helsinki.
Informed Consent
Not applicable
Data Availability
The data supporting the findings of this study are available with all authors but not publicly available due to confidentiality restrictions. However, available up on reasonable request.
Funding
None
Conflict of Interest
None