Introduction
Chronic osteomyelitis is a long-lasting bone infection that can be very painful and debilitating. It is still a major public health issue, especially in places with fewer resources.1 It usually occurs after an acute infection or inadequately managed traumatic wounds. If it is not treated quickly and adequately, it can cause long-term impairment, potential amputation, and a lower quality of life. The burden is especially heavy in Sub-Saharan Africa, where getting timely diagnosis, surgery, and follow-up care is hard.2 In these situations, the shift from acute to chronic osteomyelitis is often caused by delays in diagnosis, broken referral systems, and a lack of community knowledge.3
Several studies have investigated treatments for persistent osteomyelitis, and some treatments have worked better than others. In resource-rich settings, treatment usually includes a mix of surgery to remove dead tissue, long-term antibiotic treatments, and imaging modalities to monitor disease progression.4 However, these methods take a lot of resources and are sometimes hard to get to in rural or low-income areas. In places with few resources, some medical professionals suggest using simplified treatment algorithms and community-based screening procedures as possible options.5 A study in Uganda has shown that using basic clinical criteria and plain radiographs together for diagnosis is helpful. It also stressed the importance of getting the community involved early and providing follow-up care in a decentralized way.6 Still, the lack of standardized screening instruments and referral systems makes it hard to consistently use and scale up these kinds of interventions in rural areas.
In Rwanda, rural areas have trouble dealing with osteomyelitis because of problems with the system. Primary care clinicians sometimes do not have the specialist training or standard tools needed to make early diagnoses.7 Also, patients often present late due to limited awareness of early symptoms and barriers to accessing specialized care. In this situation, persistent osteomyelitis not only causes unnecessary illness but also puts increased pressure on health systems that are already short on resources.
It is very important to find osteomyelitis cases early and send patients to the right doctor to avoid long-term problems.8 However, there is not much research on scalable, community-driven methods that work well in rural Africa. To fill this gap, a team of experts from several fields in the Nyamasheke District developed and tested a whole intervention to stop chronic osteomyelitis by finding it early and making care easier.
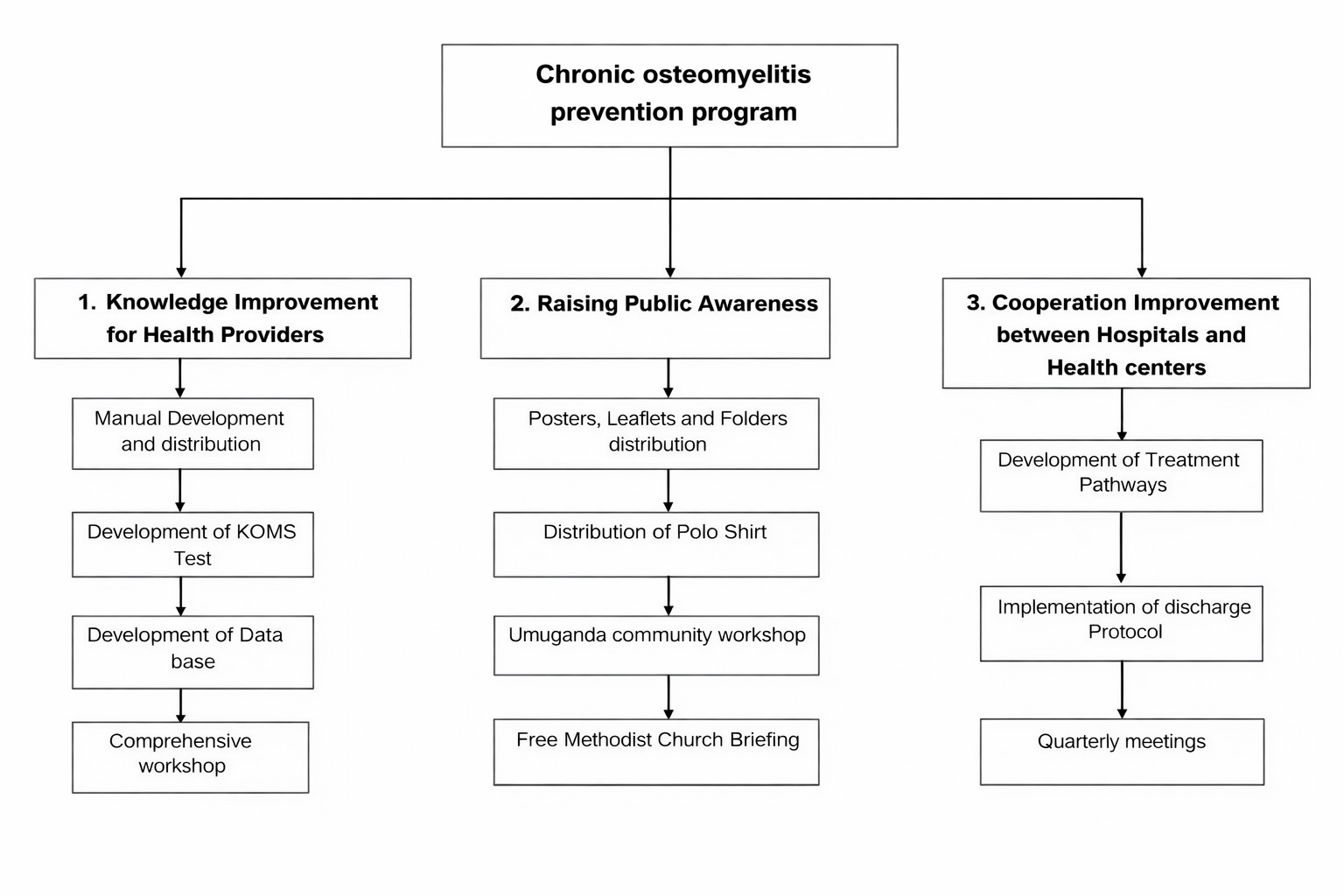
The intervention was based on three main ideas: (1) improving the knowledge and diagnostic skills of health professionals through targeted training and the creation of the Kibogora Osteomyelitis Screening Test (KOMS-Test); (2) raising awareness in the community using health promotion materials that are culturally appropriate; and (3) improving cooperation between health centers and hospitals by creating referral pathways, treatment protocols, and structured discharge processes.
This study evaluated a community-driven osteomyelitis prevention intervention in the Nyamasheke District of Rwanda. Specifically, we assessed (1) changes in the proportion of acute vs chronic osteomyelitis presentations, (2) implementation fidelity indicators (use of KOMS-Test, referrals, discharge letters, and treatment protocols), and (3) diagnostic performance of the KOMS-Test using referral hospital confirmation as the reference standard.
Materials and Methods
Study design and setting
The study used a quasi-experimental, community-based approach in the Nyamasheke District of Western Rwanda. The intervention took place over the course of two years from May 1, 2021 to June 30, 2023. The area has 20 health facilities, 2 hospitals (Kibogora and Bushenge), and a network of community health workers (CHWs). This makes it a good place to test out an integrated osteomyelitis prevention program.
Study setting
The Nyamasheke District is located in the Western Province of Rwanda and is predominantly rural with a population of 434,221 inhabitants according to the 2022 national census. The district is characterized by dispersed settlements, mountainous terrain, and limited transport infrastructure, all of which are factors that constrain timely access to specialized surgical and diagnostic services. Health care delivery in Nyamasheke relies largely on primary health centers supported by CHWs, with referral hospitals serving wide catchment areas. These structural and geographic challenges contribute to delayed presentation of musculoskeletal infections, including osteomyelitis, and increase the risk of progression from acute to chronic disease. As such, Nyamasheke represents a typical rural, low-resource context where community-based early detection and referral interventions are particularly relevant.
Study population and inclusion criteria
The study involved osteomyelitis patients and health care providers from the Nyamasheke District. Eligible participants included diagnosed patients and providers engaged in osteomyelitis care. All patients presenting with suspected or confirmed osteomyelitis at Kibogora Hospital during the study period were included in the program database. Health care providers and CHWs involved in program activities were included for implementation metrics.
Data collection subsection
At Kibogora Hospital, osteomyelitis diagnosis was confirmed by senior surgeons using clinical evaluation combined with radiographic imaging. Surgical findings were used to support diagnosis in patients undergoing operative management.
Program development process
In April 2021, a big planning session brought together 11 professionals, including orthopedic surgeons from Germany and Rwanda, general surgeons, nurses, and a public health expert. The goal of this joint workshop was to develop an intervention that will work in the region based on its epidemiology and health system facts.
The workshop led to the creation of a model with three parts:
-
Improving health care provider knowledge,
-
Raising public awareness,
-
Strengthening cooperation between hospitals and health centers.
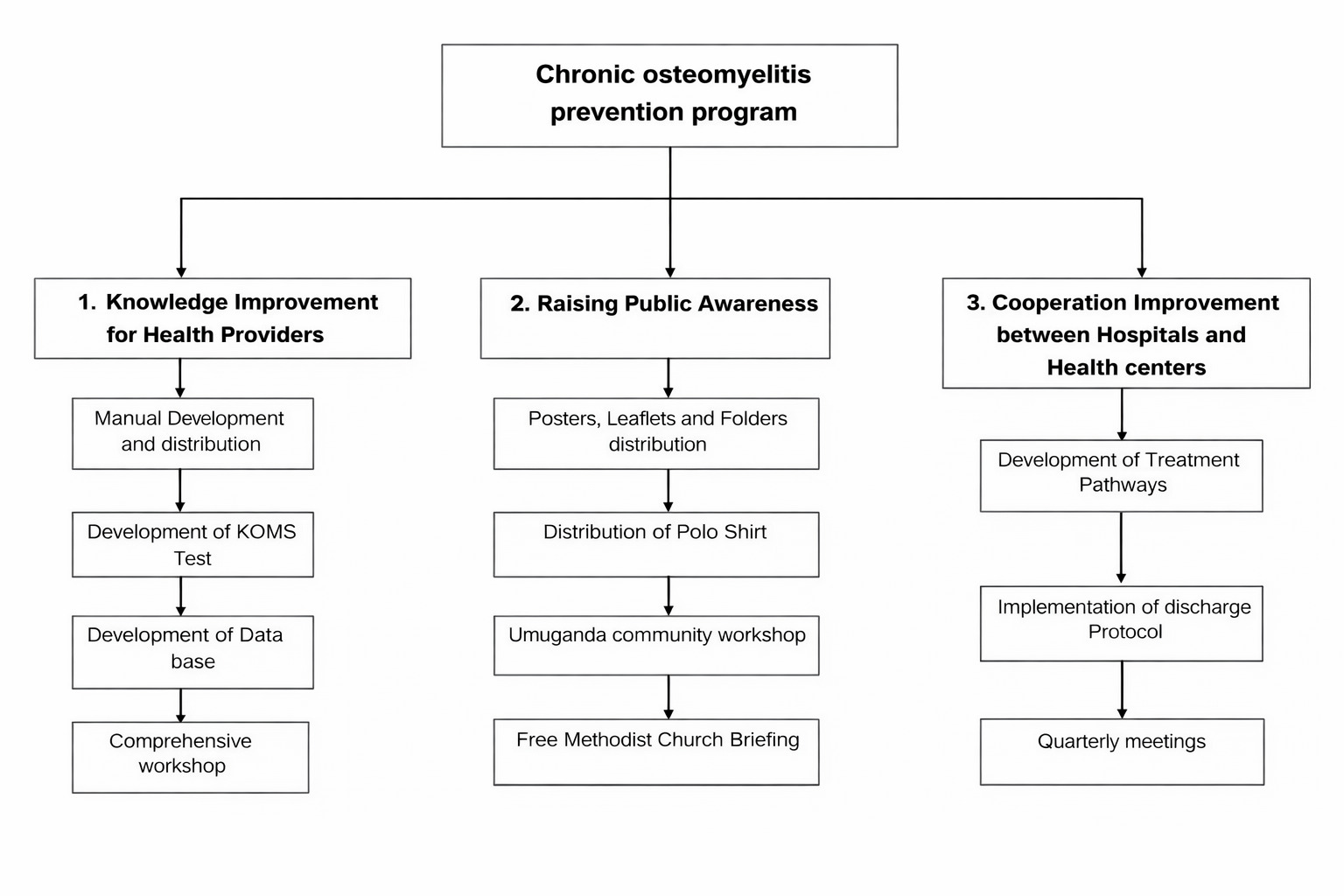
The intervention model was supported by the development of tailored materials, including a screening tool (KOMS-Test), clinical management pathways, discharge templates, and health promotion materials (Figure 1).
Development of KOMS-Test
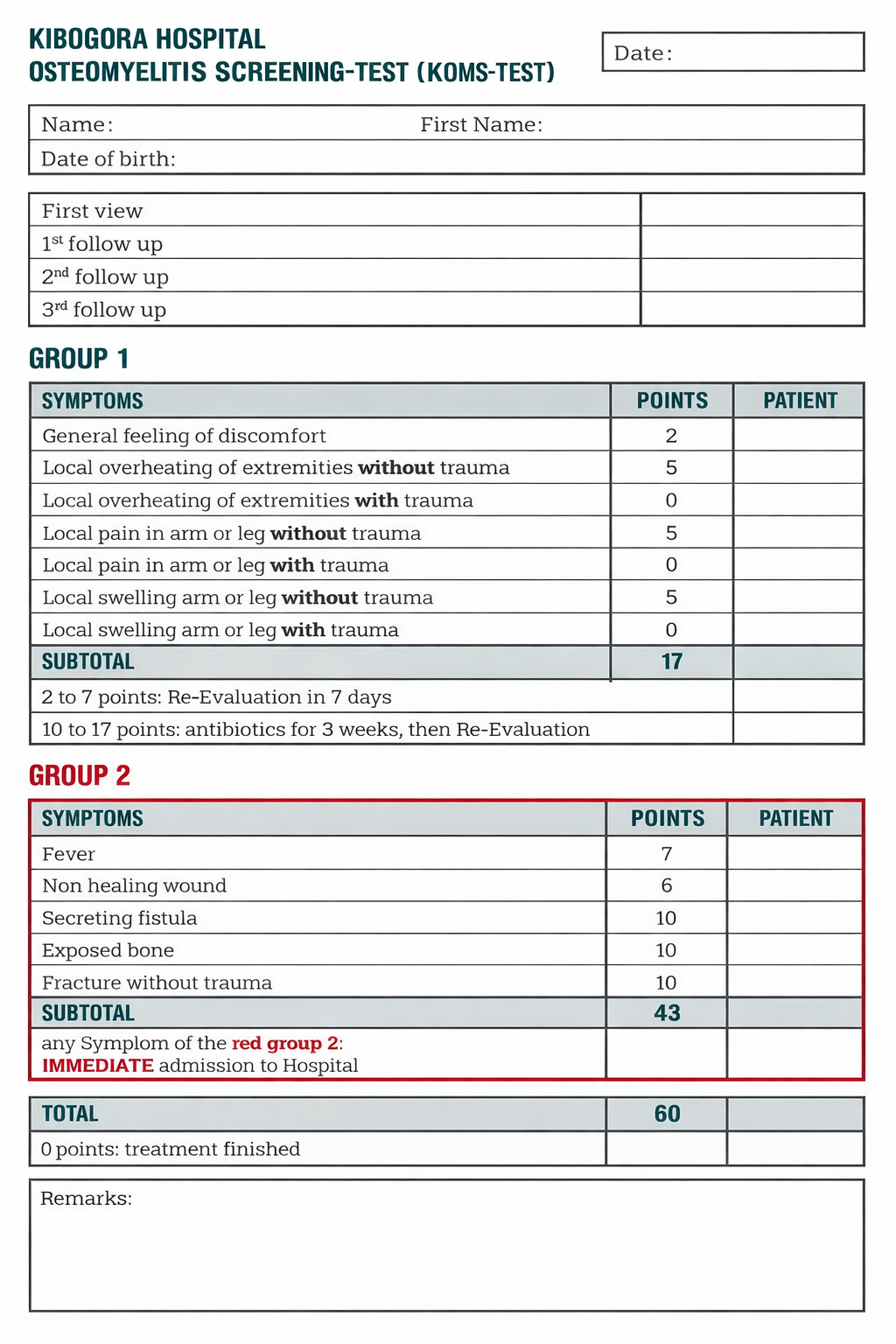
The KOMS-Test (Figure 2) was developed to address the absence of practical, standardized screening tools for early osteomyelitis detection at the primary health care level in rural settings. The tool was developed during a multidisciplinary workshop involving orthopedic surgeons, general surgeons, nurses, and public health specialists from Rwanda and Germany. Item selection was informed by clinical experience, literature on early osteomyelitis presentation, and expert consensus. Clinical signs and risk factors were assigned weighted scores to reflect their relative likelihood of osteomyelitis. Group 1 parameters capture clinical risk factors, while Group 2 parameters reflect active clinical manifestations suggestive of established infection.
_format.png)
Scoring rationale clarification (KOMS-Test)
Lower scores were assigned to nonspecific symptoms or those commonly associated with noninfectious trauma, while higher scores were allocated to features more strongly associated with osteomyelitis. Trauma-related pain or swelling without additional inflammatory or systemic features were assigned zero points to minimize false-positive referrals. The KOMS-Test was refined following preliminary field use during early implementation phases, during which wording and scoring thresholds were adjusted to improve clarity and usability at the health-center level.
Intervention components
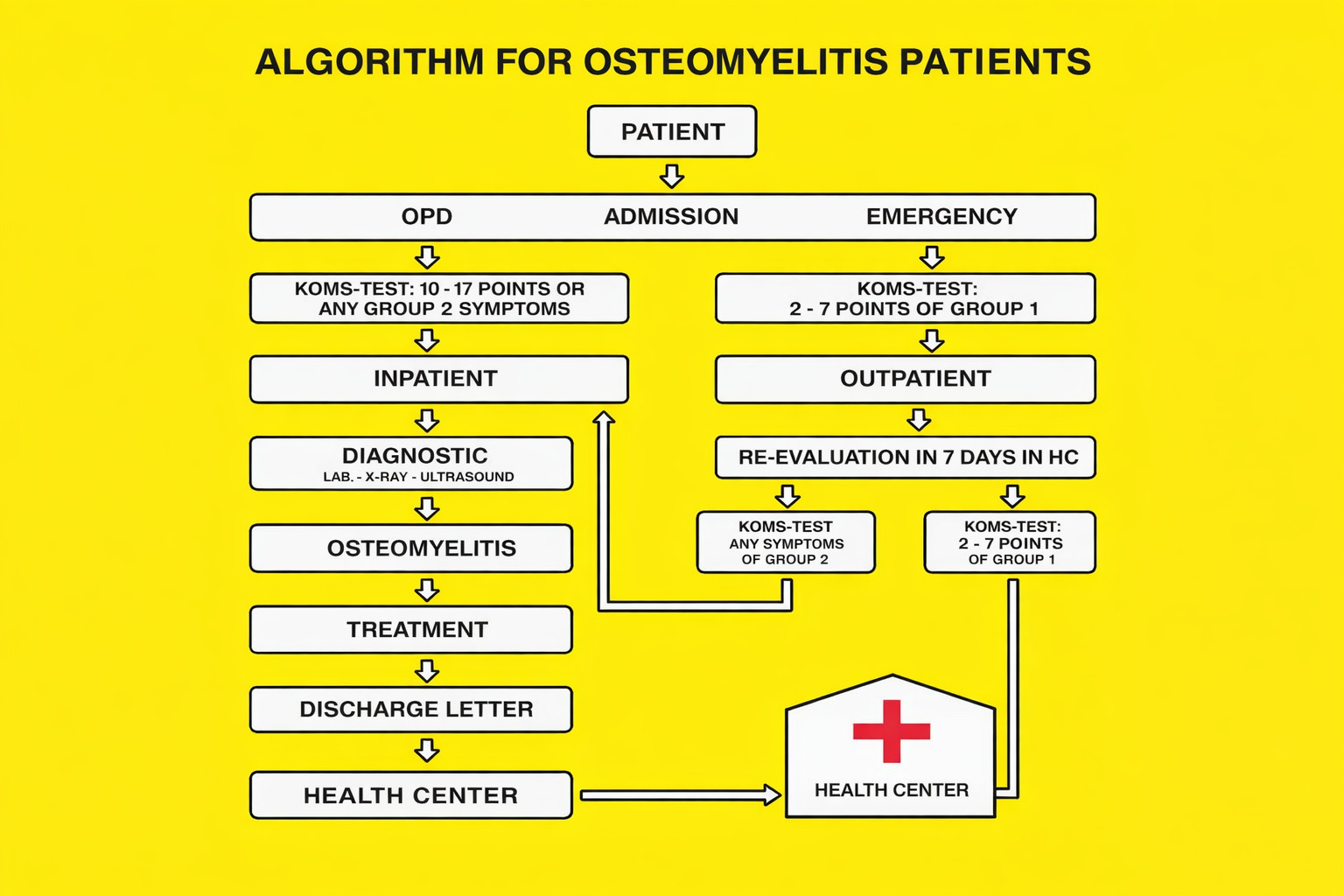
KOMS-Test utilization was defined as documented use of the screening tool during patient assessment at the health-center level. Referral compliance was defined as presentation at the referral hospital within two weeks of referral. Discharge protocol adherence was assessed through review of completed standardized discharge letters (Figure 3).
Knowledge improvement for health providers
There were 15 pages of training material on osteomyelitis written in English and then translated into Kinyarwanda. The guidebook has simplified clinical classification systems adapted from the Comprehensive Rural Surgery model, emphasizing simplified clinical decision-making, decentralization of care, and structured referral pathways suitable for low-resource settings. The KOMS-Test is a new clinical screening tool that uses a symptom-based scoring system to help primary care doctors find osteomyelitis early.
Training sessions were conducted across three cycles and targeted medical staff at all health facilities within the district. In total, 7459 training interactions were recorded, including 152 hospital staff, 1555 nurses from health centers, and 5752 CHWs. The training covered early clinical signs, the use of KOMS-Test, diagnosis, imaging interpretation, and the application of treatment pathways. A training interaction was defined as one participant attending one training session (one attendance event). Repeat attendance by the same participant was counted as separate interactions.
A training interaction was defined as a single attendance event by a health care provider or CHW at a structured training session. Repeat attendance by the same individual across sessions was counted as separate interactions.
Public awareness campaign
Educational materials were developed and disseminated to the public, including:
-
5000 informational leaflets,
-
144 posters in four sizes,
-
5 large banners,
-
2300 polo shirts with clinical pictograms for CHWs.
Community sensitization occurred during Umuganda (monthly national community service events) and through partnerships with the Free Methodist Church. Messaging emphasized early symptoms (pain, swelling, overheating, and fever) and the importance of seeking prompt medical care.
Cooperation between hospitals and health centers
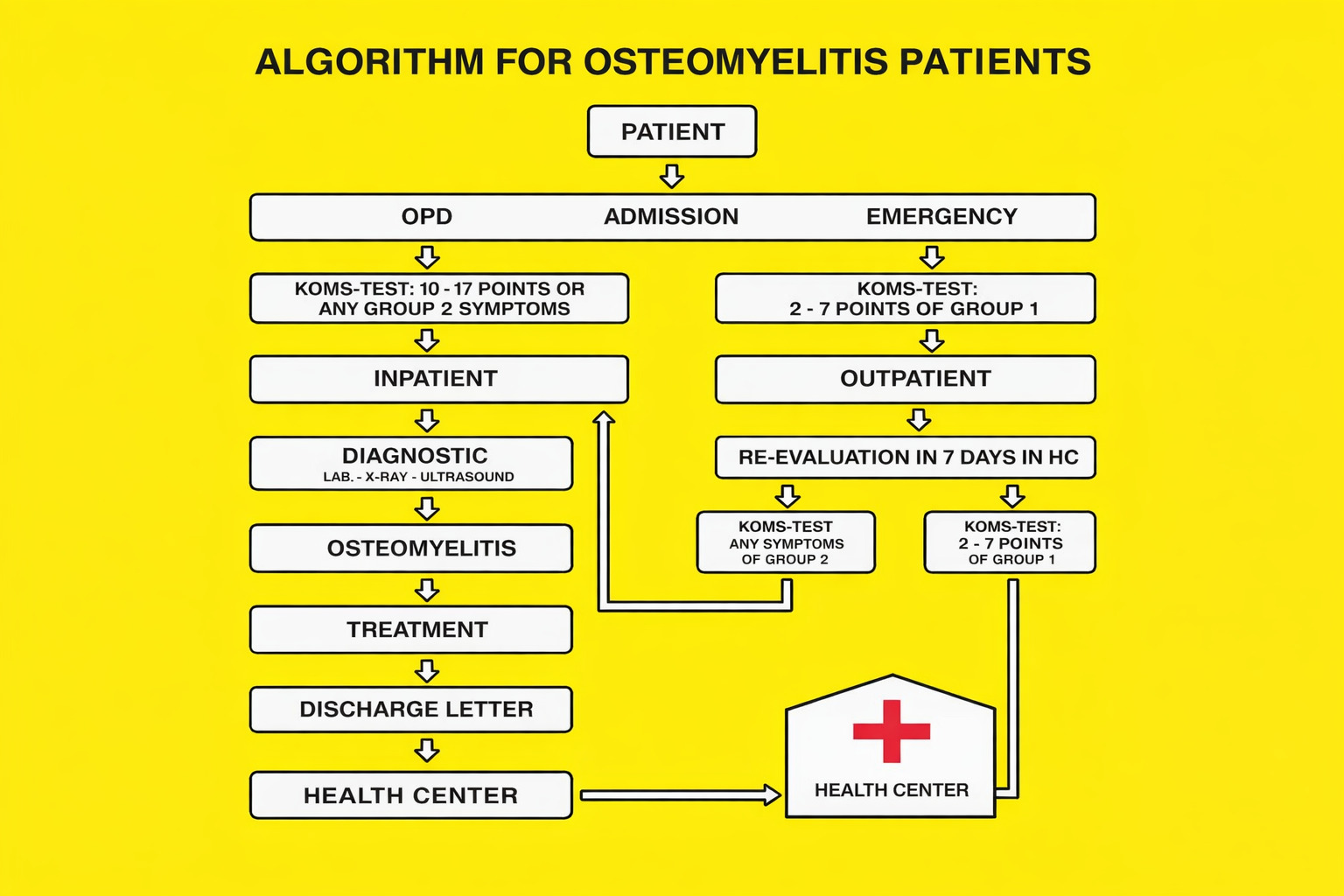
A standardized algorithm and clinical management pathway were developed to streamline the referral and treatment of osteomyelitis patients. Key components included:
-
Referral criteria based on KOMS-Test scoring,
-
Structured discharge letters specifying diagnosis, therapy, medications, and follow-up schedule,
-
Quarterly multidisciplinary meetings involving physicians, nurses, and CHWs,
-
A centralized Excel database for tracking patient data updated by data managers at Kibogora Hospital.
Patient enrollment and data collection
All patients presenting with suspected or confirmed osteomyelitis between May 1, 2021 and June 30, 2023 were included in the program database. A total of 256 cases were documented. Data were collected on age, gender, place of residence, clinical classification (acute vs chronic), severity level, KOMS-Test usage, referral pathway, hospitalization frequency, and outcomes.
Patients were stratified by origin:
-
Intervention group, which consists of patients from Nyamasheke District (trained health providers),
-
Comparison group, which consists of patients from neighboring districts (nontrained facilities).
Data analysis
We employed descriptive statistics to summarize the characteristics of the patients and the program indicators. We used chi-square testing to see if there were any changes in how groups and phases classified osteomyelitis as acute or chronic. We checked the accuracy of the KOMS-Test by determining if it was correctly used at the hospital level. We calculated the rates of use, adherence to discharge protocols, and compliance with referrals as percentages. There were few missing values, and for categorical analyses, they were dealt with by deleting the entire list. For continuous variables with missing entries, mean imputation was used when it made sense. Microsoft Excel and SPSS Version 21 were used for all analyses.
Case definitions
Chronic osteomyelitis cases were classified as simple, difficult, or complex based on the extent of bone involvement, presence of sinus tracts, history of prior surgery, and soft-tissue compromise.
Results
Patient demographics and disease characteristics
Between May 1, 2021 and June 30, 2023, a total of 256 patients were treated for osteomyelitis at Kibogora Hospital. Of these, 158 (61.7%) were male and 98 (38.3%) were female. The majority (87.9%) resided in rural areas. Age distribution revealed that 22% were between 1–10 years, 36% were between 11–20 years, 17% were between 21–30 years, and 25% were above 30 years. Half of the patients (128) presented with acute osteomyelitis, while the remaining 50% were diagnosed with chronic forms (Table 1).
Impact of the prevention program
Out of 172 patients from Nyamasheke District (intervention group), 101 (58.7%) had acute osteomyelitis and 71 (41.3%) had chronic cases. In contrast, among the 84 patients from neighboring districts (nonintervention group), only 27 (32.1%) presented with acute osteomyelitis while 57 (67.9%) had chronic forms. The difference between the groups was statistically significant (χ² = 5.23, P < 0.001), demonstrating the impact of early detection efforts (Table 2).
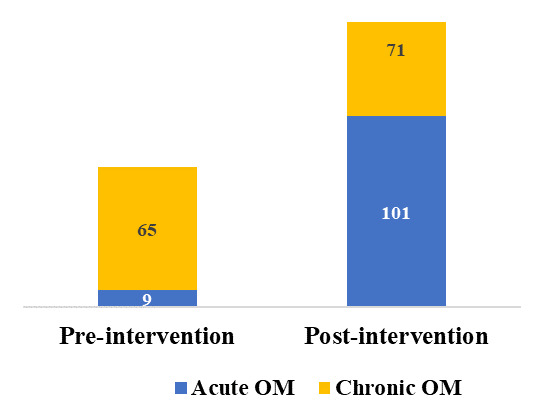
Pre- and postintervention comparison within Nyamasheke
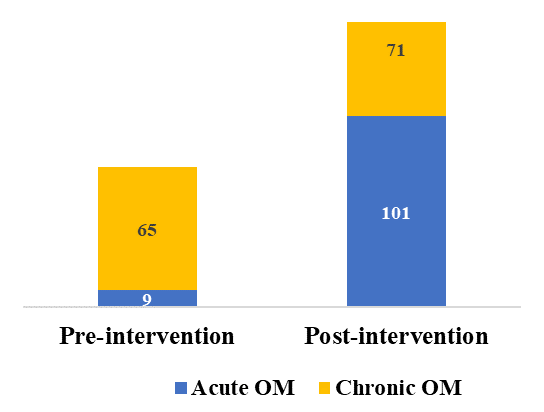
Before program implementation (Phase I), only 9 of 74 osteomyelitis cases (12.1%) were acute. After intervention (Phase III), this figure rose to 101 of 172 cases (58.7%). Chronic cases decreased from 87.9% to 41.3% (χ² = 62.34, P < 0.001) (Figure 4).
Severity and hospital readmission
Among chronic cases, 54 were simple, 62 were difficult, and 12 were complex. In the intervention group, 22.7% had difficult or complex cases vs 42% in the control group. Second hospitalization was required in 16.8% of Nyamasheke patients, compared to 29.8% in nonintervention districts (Table 3).
Screening and diagnostic performance of KOMS-Test
Among 100 patients screened using the KOMS-Test and referred to Kibogora Hospital, 97 were confirmed to have osteomyelitis, which corresponds to a positive predictive value of 97%.
Discussion
This study presents the design, implementation, and evaluation of a community-driven osteomyelitis prevention program in a low-resource, rural setting in Rwanda. The results demonstrate the feasibility and effectiveness of combining health care provider training, community engagement, and structured referral systems to reduce the burden of chronic osteomyelitis. Compared with hospital-centered diagnostic approaches, the KOMS-Test offers a low-cost, symptom-based screening method that can be implemented by nonspecialist health workers to enable earlier referral and reduce progression to chronic disease.
Our findings indicate a substantial increase in the proportion of acute osteomyelitis cases (from 12.1% to 58.7%) and a corresponding decline in chronic presentations in the intervention district, which suggests improved early detection following implementation. This aligns with earlier evidence that timely diagnosis and intervention are critical for preventing progression to chronic disease.9,10 In low-resource settings, where advanced diagnostics and surgical interventions are often unavailable, frontline detection tools, such as the KOMS-Test, offer a practical and impactful alternative.11
The high predictive accuracy of the KOMS-Test (97%) demonstrates the value of symptom-based, context-adapted screening tools. Similar efforts in Ethiopia show that simplified diagnostic algorithms, when integrated into primary care, can substantially improve case identification and triage.12 Our results contribute to this growing body of literature by demonstrating successful implementation at scale across 20 health centers in a real-world setting.
Health system strengthening was another cornerstone of this intervention. Issuing standardized discharge letters (97.2% compliance) and using clinical pathways enhanced continuity of care and coordination between hospitals and peripheral health centers. These strategies are consistent with best practices in integrated care models and are associated with improved outcomes in other chronic disease programs.13
Public awareness also played a pivotal role. The widespread distribution of leaflets, pictogram-based posters, and polo shirts contributed to heightened recognition of early symptoms by both patients and CHWs. Incorporating visual tools is also particularly important in populations with limited literacy and has been shown to improve community-level engagement in disease prevention.14
Furthermore, the program’s impact extended to disease severity and health care utilization. The proportion of patients with difficult or complex chronic osteomyelitis was significantly lower in the intervention district (22.7%) compared to neighboring districts (42.0%), and rehospitalization rates were correspondingly reduced. These outcomes suggest not only earlier detection but also more effective primary-level management. Similar results were observed in decentralized tuberculosis programs, where local detection and adherence support reduced complications and readmissions.15
This study also reinforces the importance of capacity building. Over 7000 training interactions were recorded with consistent content delivery across facility levels. Multicycle training ensured that knowledge was retained and operationalized over time, addressing a common limitation in short-term interventions. Regular multidisciplinary meetings provided a platform for iterative feedback and continuous improvement, a best practice recommended by WHO for community-based care models.16
This study provides compelling evidence that context-specific, community-based interventions can significantly improve the early diagnosis and management of chronic osteomyelitis in low-resource settings. The structured integration of training, awareness campaigns, and referral systems represents a replicable model that may be scaled to other rural districts in Rwanda and beyond.
Although the KOMS-Test demonstrated a high positive predictive value among referred patients, comprehensive diagnostic validation, including sensitivity, specificity, and receiver operating characteristic analysis, could not be performed due to limited follow-up of screen-negative cases. Further prospective validation is warranted. This manuscript presents early implementation and performance data that support the potential utility of the KOMS-Test in low-resource settings. These findings should be considered hypothesis-generating and provide a foundation for future validation studies aimed at broader adoption.
Conclusion
This study demonstrates the feasibility and impact of a context-adapted, community-driven intervention aimed at preventing chronic osteomyelitis in a low-resource setting. Through the integration of a simplified clinical screening (KOMS-Test), provider training, public awareness, and structured referral and treatment pathways, the program significantly increased the proportion of acute osteomyelitis cases detected and reduced chronic complications. The high utilization and predictive accuracy of the KOMS-Test, combined with strong adherence to clinical protocols, reflects a health system capable of operationalizing low-cost, scalable solutions. These findings support the adoption of community-based early detection models for musculoskeletal infections in similar rural and underserved regions globally.
Study Limitations
This study has the following limitations. While a comparison was made with neighboring districts, the absence of randomization or baseline matching limits causal attribution. Also, outcome validation was dependent on radiographic and clinical diagnosis at a single referral hospital, which may introduce diagnostic variability. Additionally, long-term follow-up beyond the program period was not conducted, making it difficult to assess relapse rates or sustained community behavior change. Future research should consider prospective study designs, multisite evaluations, and cost-effectiveness analyses to strengthen generalizability and policy relevance. Patients scoring below the KOMS-Test referral threshold were managed conservatively at the health-center level and were not routinely followed to assess false-negative outcomes, which limit estimation of sensitivity and negative predictive value.
Acknowledgments
The authors wish to acknowledge the contributions of the staff at Kibogora and Bushenge Hospitals, the CHWs in Nyamasheke District, and the patients who participated in this program. Special thanks to Kibogora Polytechnic University for institutional support.
Ethical Approval
Ethical approval for this study was obtained from the Rwanda National Ethics Committee (RNEC) (IRB No: 00001497; IORG No: 0001100).
Informed Consent
Written informed consent was obtained from all participants or their legal guardians prior to data collection and participation in training or evaluation activities.
Data Availability
The datasets used and analyzed during the current study are not publicly available due to institutional restrictions, but they are available from the corresponding author upon reasonable request.
Conflict of Interest
The authors declare that they have no competing interests.
Funding
This work did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.