Introduction
Trauma remains a leading global cause of morbidity and mortality, particularly among individuals 45 years and younger.1–5 Hemorrhagic shock resulting from uncontrolled exsanguination accounts for nearly half of trauma-related deaths within the first 24 hours, with a substantial proportion occurring during the initial 2–3 hours following injury.6,7 Prompt recognition and resuscitation are critical to improving survival by preventing the progression of the lethal triad: hypothermia, acidosis, and coagulopathy.2,8–10
Standard shock classification as described in Advanced Trauma Life Support guidelines remains central to trauma assessment. However, estimation of blood loss and reliance on individual physiological parameters may be influenced by compensatory mechanisms in early shock, and volume loss is often difficult to quantify instantaneously.11,12 While serum lactate level is a reliable biomarker for hypo-perfusion, testing for it is often unavailable in trauma centers located in low- and middle-income countries (LMIC).13 Trauma severity scoring systems like the New Injury Severity Score (NISS) and Revised Trauma Score (RTS) have demonstrated utility for prognostication, but their dependence on comprehensive diagnostics limits their application in many LMICs.14
In this context, composite measures such as the Shock Index (SI), defined as the ratio of heart rate to systolic blood pressure, with a normal range of 0.5 to 0.7, may provide an additional simple, rapid, and noninvasive indicator of early hemodynamic compromise.2,8 The application of SI in trauma triage across the sub-Saharan region remains limited, and it is rarely integrated into routine clinical practice or national treatment protocols.15–18 LMICs, including Tanzania, experience challenges in trauma care from limited pre-hospital services, delayed imaging and laboratory diagnostics, and inadequate care infrastructure.19,20
The prognostic utility of SI in obstetrics, cardiovascular emergencies and trauma has mostly been demonstrated by retrospective studies originating from high-income countries.21 There is also a marked paucity of prospective research on patterns of trauma with elevated SI within sub-Saharan Africa, where trauma systems face unique resource and infrastructure constraints.22
This study aims to address existing regional gaps by examining the proportion and clinical characteristics of trauma patients presenting with hemodynamic compromise or instability (SI >0.7) at a national referral center in Tanzania. It further assesses how varying levels of elevated SI correlate with injury severity, trauma scores (NISS and RTS), and short-term outcomes. Additionally, the study identifies predictors of mortality and prolonged hospitalization among patients with elevated SI to support early risk stratification in resource-limited settings.
Methods
Study site, design and settings
This was a prospective, observational cohort study conducted between June and September 2024 at a high-volume, tertiary national trauma referral center in an urban area of Dar es Salaam, Tanzania. The center functions as one of the country’s primary facilities for orthopedics, trauma, and neurosurgery, serving a catchment population exceeding 10 million. It operates a 24-hour emergency department (ED) staffed by specialist trauma personnel and manages approximately 4000 outpatient visits and 110 inpatient admissions weekly.
Study population and eligibility criteria
All adult trauma patients (aged ≥18 years) presenting at the ED during the study period with a SI >0.7 were eligible. The threshold of >0.7 was selected because it exceeds the upper limit of normal physiological range (0.5–0.7) and reflects early hemodynamic compromise, thereby allowing identification of patients at risk of clinical deterioration. Exclusion criteria included known cardiac disease, pacemaker use, ongoing ionotropic or chronotropic medication, pregnancy, confirmed infection, death on arrival, or prior major surgical intervention or hospital care before referral. These exclusions were applied to minimize non-trauma related physiological modifiers confounding heart rate and blood pressure responses, thereby preserving the interpretive validity of SI as a marker of trauma-induced hemodynamic compromise. All included patients sustained blunt trauma, without penetrating injuries. Informed consent was obtained from all participants or their proxies.
Sampling and data collection
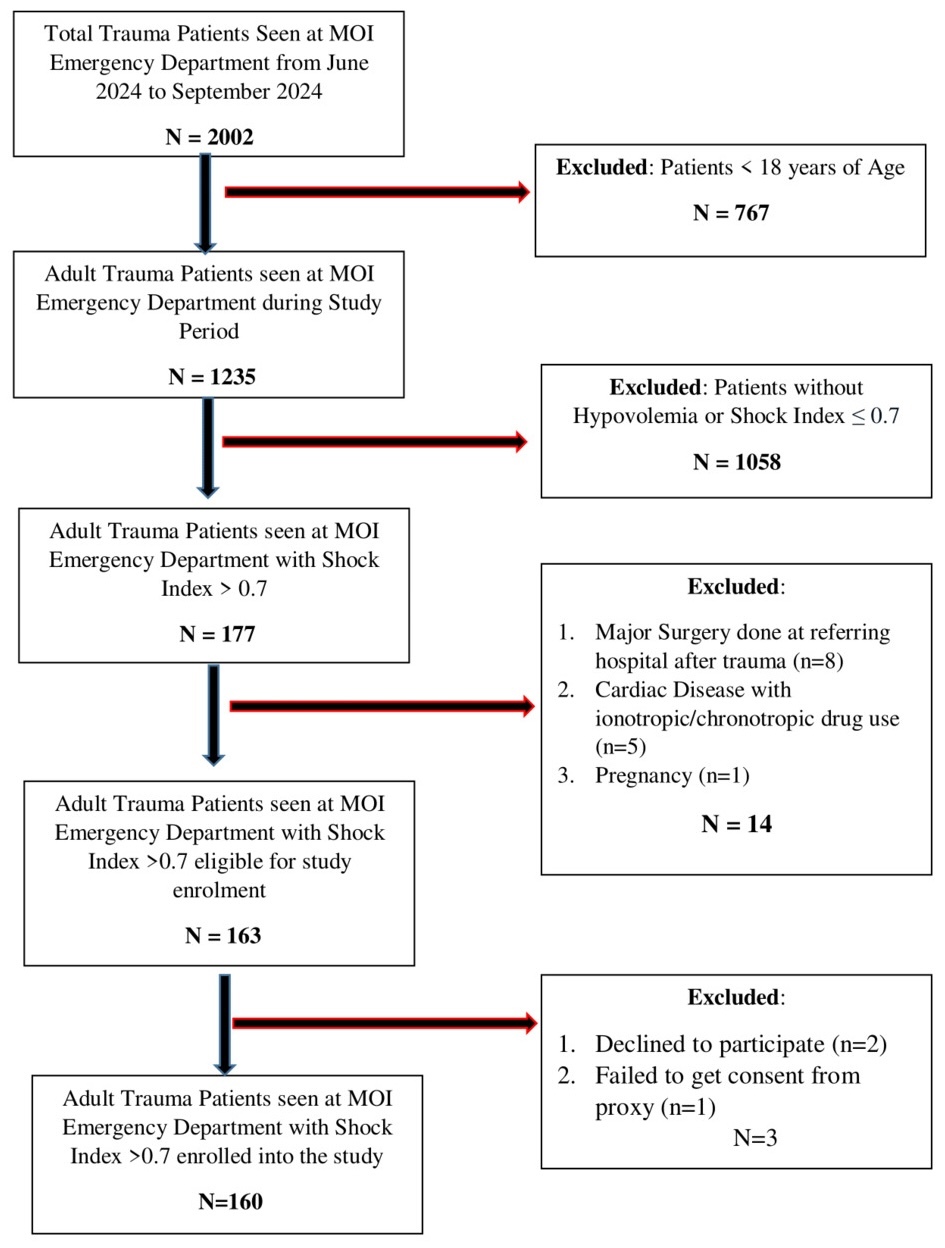
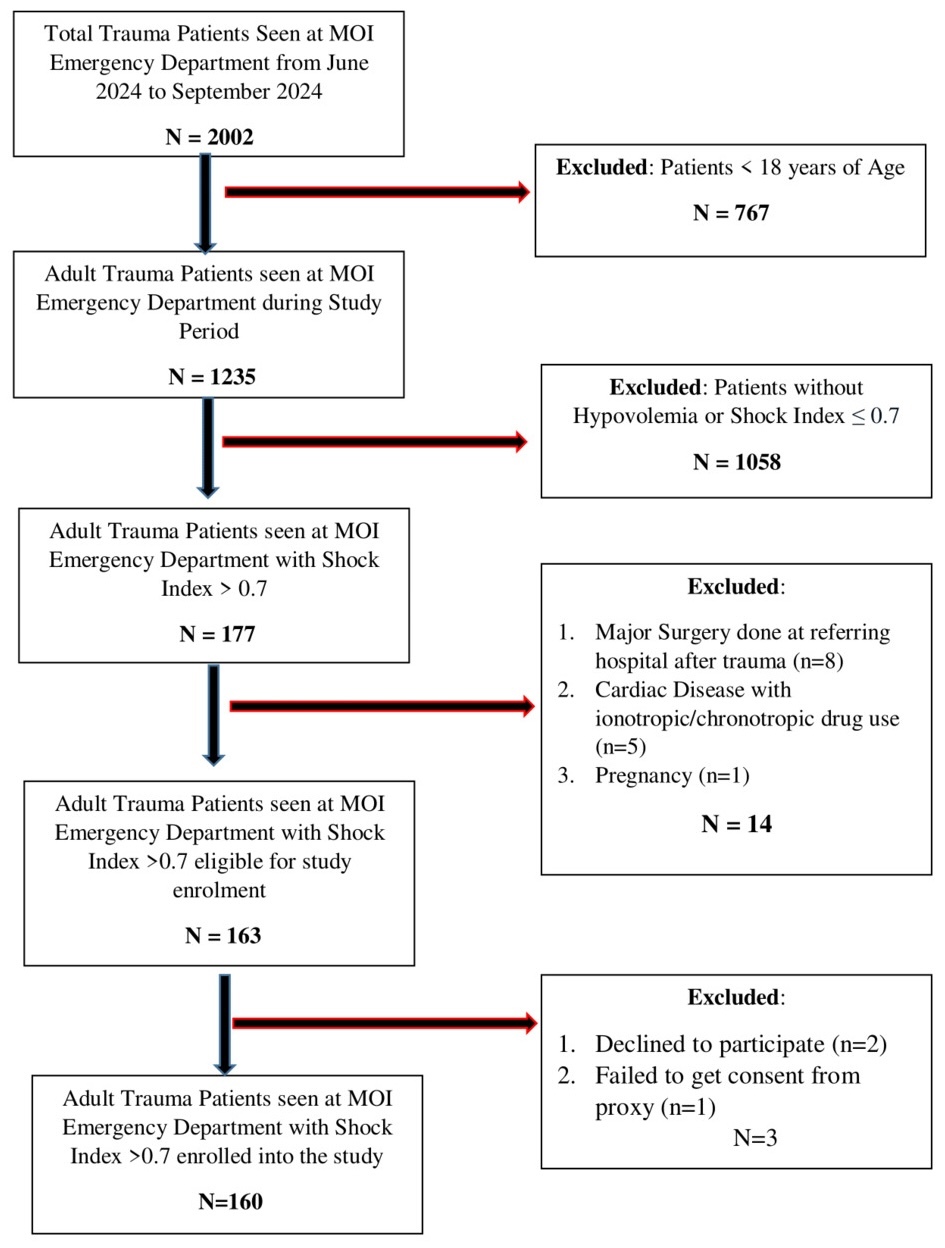
Patients were recruited using consecutive sampling. Trained research personnel used a structured data collection tool to prospectively gather data, including brief patient history (including age and mechanism of injury) alongside clinical records and assessments. Eligible patients were identified immediately upon arrival at ED triage area, irrespective of time of presentation. Research assistants worked in shifts to ensure continuous recruitment, and patients for whom consent could not be obtained were excluded (Figure 1).
During casualty department triage assessment, demographic variables and injury mechanisms and patterns were recorded and verified with attending clinicians. Baseline clinical data at patient arrival, before initiation of resuscitative interventions, were obtained from ED triage records. Data included heart rate, systolic blood pressure, respiratory rate, GCS, and hemoglobin level. Patients were followed for 7 days after admission to assess early outcomes.
Study variables and measures
Primary variables included SI, NISS, and RTS. Secondary variables were age, sex, mechanism of injury, hemoglobin level, and the count and location of significantly injured anatomical regions.
A significant injury was defined as one of at least moderate severity, requiring medical intervention and corresponding to an Abbreviated Injury Scale (AIS) score of ≥2. NISS, which quantifies anatomical injury, was computed by squaring and summing the three highest AIS scores.
Hemoglobin level was recorded from the first laboratory sample obtained at presentation to the casualty department, with laboratory services available continuously. Values were recorded as continuous variables and classified as anaemic or non-anaemic according to World Health Organization hemoglobin thresholds for adults (hemoglobin <13.0 g/dL in males and <12.0 g/dL in females).
Weighted RTS, a physiological scoring system, was calculated using GCS, systolic blood pressure, and respiratory rate. For analytical purposes, SI was categorized into low (SI<1) and high (SI≥1) cohorts, consistent with established literature identifying SI ≥1 as a threshold associated with increased risk of decompensation and mortality.
The primary outcomes were mortality and length of hospitalization (≤7 days vs >7 days). A threshold of 7 days was selected to reflect the intensity of early inpatient care after trauma and to capture clinically meaningful short-term hospital utilization. Longer-term data is often difficult to obtain in our setting because patients are often lost to follow-up after their initial stabilization and discharge.
Bias mitigation
Selection bias was minimized through consecutive, nonselective patient enrollment and predefined eligibility criteria. Patients with comorbidities or prior trauma surgical care were excluded to reduce confounders from treatment. Standardized data collection tools and validated trauma scores (SI, NISS, RTS) were used. Anatomical injury scoring was independently verified by surgical specialists and radiologists to reduce measurement bias. This study was conducted at an orthopedic and trauma national referral center where attending-level oversight is mandated for all admitted patients as part of routine institutional policy.
Data management and statistical analysis
Data were double-entered into Excel, Version 2019 (Microsoft Corporation, Redmond, WA, USA) and analyzed using SPSS Statistics for Windows, Version 25.0 (IBM Corp, Armonk, NY, USA) and RStudio Version 2024.03.0+492; R version 4.3.2 (RStudio, PBC; Boston, MA, USA). Continuous variables were summarized using means and standard deviations or medians and interquartile ranges, as appropriate. Categorical variables were presented as frequencies and percentages. Bivariate analysis was performed using chi-square and Fisher’s exact tests for categorical variables and independent t tests, and the Mann-Whitney U (Wilcoxon) test for continuous variables. Relative risks (RR) with 95% confidence intervals (CI) were calculated. A two-tailed P value ≤.05 was considered statistically significant. SI was also dichotomized into low (SI <1) and high (SI ≥1) categories for subgroup analysis.
Multivariable logistic regression was performed to identify independent predictors of mortality within 7 days and prolonged hospitalization. Variables with P ≤.20 on univariate analysis, as well as those considered clinically relevant from prior literature, were entered into the model. A forward stepwise (likelihood ratio) approach was used for variable entry and retention. Adjusted odds ratios (AOR) with 95% CI were reported, and statistical significance was set at P ≤.05.
Results
Demographic and clinical characteristics
From June 1st to September 30th 2024, 1235 adult trauma patients presented to the ED, and 160 (13%) met eligibility criteria for elevated SI (SI >0.7) indicating hemodynamic instability (Figure 1). Among them, 61 (38.1%) demonstrated markedly elevated SI (SI ≥1). Median age did not differ significantly between the high- and low-SI cohorts (35.0 vs 34.2 years, P = .676), and age distribution was similar (P = .961). Males were significantly more likely to present with high SI than females (41.8% vs 19.2%, P = .045; RR = 2.17, 95% CI: 0.96–4.90).
High SI was associated with greater injury severity. Patients with SI ≥1 were more likely to have NISS >15 (64.1% vs 35.9%, P <.0001; RR = 21.8), RTS <6 (76.5% vs 23.5%, P = .0015; RR = 2.28), and GCS ≤8 (75.0% vs 25.0%, P = .0022; RR = 2.20). Anemia was also more prevalent among high SI patients (50.9% vs 13.0%, P <.0001; RR = 3.93) (Table 1).
Injury mechanisms, distribution, and early outcomes
Motor traffic crashes were the most common injury mechanism in both groups, with no significant difference between high- and low-SI patients (P > .05). In contrast, injury pattern and distribution differed significantly (Table 2).
Head injuries were more frequent among high SI patients (58.2% vs 41.8%, P <.0001; RR = 3.14, 95% CI: 1.92–5.15), as were chest injuries (73.9% vs 26.1%, P = .0003; RR = 2.30) and abdominal injuries (90.9% vs 9.1%, P = .0006; RR = 2.66). Multisystem trauma was more common in the high-SI cohort; patients who sustained >3 injuries were 2.5 times more likely to present with high SI (P = .0021; RR = 2.53). The median injury count was also higher (3 vs 1, P = .0001).
Early outcomes were worse in the high SI cohort. All deaths within 7 days occurred among patients with SI ≥1 (P = .00033; RR = 27.42). Prolonged hospitalization (>7 days) was also significantly more likely (78.7% vs 21.3%, P = .00012; RR = 1.69) in this cohort.
Multivariate predictors of high SI and clinical outcomes
On multivariate analysis, three variables were associated with high SI (SI ≥1): higher NISS (AOR = 1.32, 95% CI: 1.17–1.50, P <.001), lower hemoglobin levels (AOR = 0.68, 95% CI: 0.53–0.86, P = .002), and presence of more than three injured anatomical regions (AOR = 33.97, 95% CI: 1.09–696.04, P = .044). Individual injury locations, RTS, and GCS were not independently associated with high SI. The model showed strong fit (pseudo R² = 0.498, P <.001).
Penalized logistic regression showed that high SI (AOR = 13.30, 95% CI: 1.15–3361, P = .035), low RTS (AOR = 25.89, P = .037), and low GCS (AOR = 0.39, P = .022) were significantly associated with 7-day mortality (Table 3). NISS, anemia, and injury locations lost significance after adjustment. NISS >15 (AOR = 33.48, 95% CI: 5.98–187.51, <.0001) and head injury (AOR = 1.43, 95% CI: 1.03–5.75, P = .0029) remained associated with prolonged hospital stays (Table 4). SI and other injury characteristics were not independent predictors of prolonged hospitalization (>7 days).
Discussion
This prospective observational cohort study highlights the substantial occurrence of hemodynamic compromise among trauma patients at a national referral center in Tanzania, with 13% of adult trauma admissions presenting with SI values above the normal physiological range. Retrospective studies from high-income settings have shown comparatively lower proportions of unstable patients.7 The differences are likely due to variations in pre-hospital care, trauma system maturity, and referral pathways that influence physiological status at hospital arrival.
A key finding of this study is the strong correlation between SI and established trauma severity indices, reaffirming SI as a meaningful physiological marker in the Tanzanian trauma care context. Patients with elevated SI demonstrated significantly higher NISS, indicating greater anatomical injury burden, alongside significantly lower RTS, reflecting compromised physiological reserve. This concurrent association with anatomical injury burden and physiological derangement supports the utility of SI as an early indicator of trauma-related circulatory instability.
Elevated SI was also significantly associated with lower hemoglobin levels at presentation, an effect that persisted after multivariate adjustment. This relationship may reflect reduced oxygen-carrying capacity contributing to hemodynamic compromise. In the Tanzanian context, where chronic anemia is relatively prevalent, pre-existing low hemoglobin may partially account for this finding, although differentiation from acute hemorrhage was not possible within the study design.
The use of SI >0.7 as an inclusion threshold and SI ≥1.0 for subgroup analysis aligns with established trauma literature from high-income settings. Previous studies have consistently demonstrated that SI >0.7 reflects early hemodynamic instability, while SI ≥1.0 is associated with markedly increased risks of hemorrhagic shock, transfusion requirements, physiological decompensation, and mortality.2,8,16,23,24 This two-tiered approach enabled sensitive identification of unstable patients while maintaining clinically meaningful stratification consistent with global SI research.
In this cohort, SI ≥1.0 was strongly associated with early mortality and accounted for all deaths occurring within 7 days. Multivariate analysis showed that SI ≥1.0, along with low RTS and low GCS scores, were associated with short-term mortality. These findings underscore the prognostic sensitivity of SI in identifying patients at risk of rapid physiological deterioration, even when conventional vital signs may still appear acceptable. The concentration of early mortality within the high SI group may reflect delayed recognition and stabilization of critically unstable trauma patients, a challenge commonly encountered in LMIC settings.
The strong association between SI ≥1 and early mortality in this study underscores its practical value as a frontline triage tool. In resource-limited trauma settings where delays in diagnostic imaging, laboratory testing, and specialist review are common, SI provides an immediate physiologic signal identifying patients at high risk of deterioration. The exclusive occurrence of mortality among patients with SI ≥1 suggests that this threshold could serve as a trigger for early activation of resuscitation protocols, expedited surgical evaluation for potential sources of bleeding, and prioritization for closer hemodynamic monitoring. Moreover, SI can be recalculated rapidly and repeatedly at the bedside, allowing clinicians to detect trends indicating worsening instability. Integrating SI ≥1 into triage algorithms may therefore help reduce preventable delays, ensure timely escalation of care, and optimize the allocation of limited resources such as resuscitation bays, blood products, and critical care beds.
The anatomical distribution of injuries further supports SI’s ability to identify life-threatening trauma. Patients with elevated SI were significantly more likely to have sustained injuries involving the head, chest, and abdomen, regions often affected by high-energy mechanisms and associated with occult internal bleeding. The high SI group also demonstrated significantly longer hospitalization. This finding is consistent with international studies that have reported SI thresholds ≥1 to be associated with mortality and prolonged admission.2,17,25 However, the multivariate analysis for this study showed that elevated SI was not independently associated with prolonged hospital admission. Importantly, this finding contributes evidence specific to Tanzania, emphasizing SI’s value in settings where advanced diagnostics may be delayed or unavailable.4
Demographic patterns in this study also mirror global trauma trends. Males constituted the majority of trauma victims, a pattern widely documented in trauma epidemiology.2,6–8,26 This disparity most likely reflects greater occupational exposure, engagement in high-risk activities, and disproportionate involvement in road traffic incidents. The mean age of 34.5 years highlights the heavy burden of injury among young adults, a population crucial to national productivity. Similar age distributions have been observed across LMICs, where young men commonly work in informal sectors, transport, and construction, settings associated with high trauma risk.2,3,26,27 These patterns underscore the urgent need for targeted injury prevention programs and occupational safety policies, particularly among working-age males.
Motor traffic crashes accounted for over 80% of injuries in this study, a proportion higher than that reported in many regional studies.2,15,26,28,29 This likely reflects the unique urban transport dynamics of Dar es Salaam, Tanzania, where a large proportion of young men are employed as commercial motorcycle riders (“boda boda”). The rapid urbanization, inadequate protective infrastructure, and limited enforcement of traffic regulations have contributed to the rising incidence of road traffic trauma in East Africa.30,31 These findings reinforce the need for national road safety reforms and protective legislation for high-risk transport workers.
The distribution of injuries revealed a predominance of extremity and head trauma, with more than half of patients sustaining multisystem injuries. This pattern aligns with reports from other LMIC trauma centers.1,2,14,15,20 However, injuries involving the chest, abdomen, and pelvic viscera appeared underrepresented in our cohort. This may reflect multiple factors, including referral patterns as well as pre-hospital mortality. Severe thoracic and abdominal injuries are known to carry a high risk of death before hospital arrival, even in well-resourced trauma systems. In settings with limited pre-hospital care infrastructure, this effect may be further amplified and could contribute to the injury distribution shown in this study.
Although SI is commonly used as an early marker of hemorrhagic shock, it is not specific to hypovolemia. Elevated SI may reflect other forms of hemodynamic instability, including hypovolemic, septic, obstructive, or mixed shock states. In contrast, neurogenic shock, characterized by hypotension with relative bradycardia due to loss of sympathetic tone, may result in a normal or reduced SI despite significant circulatory compromise.
Pain, anxiety, and sympathetic activation can also transiently elevate heart rate and reduce systolic blood pressure, resulting in increased SI values without significant blood loss. In this study, not all patients with elevated SI were anemic, and biochemical markers of hypo-perfusion such as lactate and base deficit were unavailable. Consequently, while high SI strongly correlated with anatomical injury severity and short-term adverse outcomes, it should be interpreted as reflecting circulatory compromise rather than as definitive confirmation of hemorrhage-driven hypovolemia.
Study strengths and limitations
A major strength of this study lies in its prospective design and use of validated trauma scoring systems: SI, NISS, and RTS, measured at the point of care. Real-time data collection in the ED and anatomical scoring confirmed by attending surgeons enhance the internal validity of our findings. To our knowledge, this is among the few prospective studies in sub-Saharan Africa assessing hypovolemic trauma using SI,4 thereby contributing important regional data that may inform trauma triage protocols and resource allocation in LMICs.
However, several limitations must be acknowledged. First, as this was a single-center study conducted at a national referral hospital, findings may not be generalizable to district-level or rural facilities where patient profiles and resource availability differ. Secondly, advanced laboratory parameters such as serum lactate and base deficit, which are valuable in shock assessment and risk stratification, were unavailable due to resource constraints.
The time interval between injury and hospital presentation was not systematically recorded, limiting assessment of pre-hospital delay and its potential influence on SI at presentation. Additionally, the very small proportion of elderly adults among the study participants limits the interpretation of SI performance in older populations, for whom predictive accuracy is known to be reduced.
Further, the relatively few outcome events, particularly mortality, may have limited the statistical stability of multivariable estimates and contributed to a wide CI. Lastly, the study’s follow-up period was limited to 7 days, so complications, disability, or mortality beyond the acute phase were unrecorded.
Conclusion
Elevated SI was common among trauma patients in this setting and served as a useful early marker of haemodynamic compromise. Higher SI values were strongly associated with greater injury severity, anemia, multisystem trauma, and early mortality. SI ≥1, together with low RTS and low GCS, independently predicted death within 7 days, underscoring the prognostic value of simple bedside evaluations in resource-limited trauma environments.
In contrast, prolonged hospitalization was determined by higher NISS and the presence of head injury, highlighting the importance of anatomical injury burden in driving recovery and resource needs. Incorporating SI into triage protocols may improve early risk stratification, while combining SI with anatomical scoring could enhance prediction of longer-term outcomes in sub-Saharan trauma care.
Ethical Approval
Ethical clearance was granted by the Muhimbili University of Health and Allied Sciences Institutional Review Board and Muhimbili Orthopaedic Institute Research Committee.
Informed Consent
Written, informed consent was obtained from all participants or their proxies. Refusal to participate did not affect patient management. The study adhered to the ethical guidelines of the Declaration of Helsinki.
Data Availability
The dataset is available from the authors upon request.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
None