Introduction
With the passage of World Health Assembly Resolution 68.15 in 2015 and the WHA73 resolutions in 2020, surgery has gained recognition as a global health priority.1,2 However, low- and middle-income countries face challenges in access, delivery, and affordability of surgical care. Specifically, countries across Africa face gaps in surgical access due to high surgical disease burden, inadequate infrastructure, low provider density, and limited financing.3,4 There is a critical shortage of surgical professionals across the continent, with only 0.5 surgeons and 0.1 anesthesiologists per 100,000 people, and a projected deficit of 6 million health workers by 2030.5,6 Thus, workforce expansion is central to improving access to surgical care and achieving universal health coverage targets.
Regulatory bodies and professional organizations have made some progress in expanding surgical care, yet past efforts were often siloed. Regional surgical societies endorse expanded partnerships to address surgical disparities more efficiently. For example, the Pan-African Surgical Healthcare Forum (PASHeF 2023) published a consensus statement on national surgical planning that revealed strong local interest in strengthening the surgical workforce.7 However, broader, multisectoral stakeholder engagement in surgical discourse is needed,
The Pan-African Surgical Conference (PASC) spanned February 24 to 28, 2025, in Kigali, Rwanda. The meeting brought together diverse stakeholders, including perioperative providers, professional societies, academia, government, and private industry, in dialogue focused on surgical workforce development. This report summarizes themes and recommendations from the meeting.
Materials and Methods
Conference preparation
A concept note was drafted by co-chairs Dr. Faustin Ntirenganya (Rwanda) and Dr. William Magee III (United States) 18 months before the meeting. Members of regional societies, academic institutions, and professional networks were invited to form an international steering committee, with specific quotas defined to ensure representation from all sub-Saharan regions (Table 1). Endorsements were received from the Ministry of Health (MOH) of Rwanda, the University of Rwanda, Rwanda Surgical Society, and Operation Smile. Financial support from organizations and industry were used to maximize stakeholder attendance by offsetting travel, accommodation, and productivity losses, which have been previously reported as barriers to scientific conference participation.8–10
The steering committee met monthly to develop the conference program. Themes were selected based on relevance to surgical workforce expansion and included surgical education, innovation, surgical ecosystems, research, and policy and advocacy. Speakers were selected based on relevant expertise, and priority was given to those based in Africa to highlight regional experiences and perspectives. Speakers and delegates from policy, multidisciplinary clinical care, academic, nongovernmental organization (NGO), and corporate/private industry backgrounds were invited to attend the meeting. Sessions were structured to include contextualizing evidence (e.g., a review of the status of surgical care in Africa relative to Global Surgery 2030 targets),11 expert panel discussions, and open discussion.
Thematic analysis and derivation of key recommendations
Artificial intelligence (AI) was utilized in compliance with TITAN Guidelines (2025) to generate draft transcriptions from audio recordings of the plenary sessions.¹² Authors (GD and LHG) recorded simultaneous field notes to capture salient quotes and time stamps. During program recruitment by conference co-chairs, speakers consented to being recorded and no personal characteristics were stated other than professional titles. These recordings did not contain personally identifiable or protected health information and were processed using Otter.ai (Otter, Otter Pro Plan, Version 3.28, 2024) via a cloud-based programming interface. The tool operated remotely and did not integrate with other software systems beyond standard cloud storage access. The transcripts were manually reviewed by 4 researchers, including male and female surgeons and public health professionals involved in global surgery and perioperative research (AU, GD, LHG, DO), who corrected transcription errors and discarded inaccuracies. Transcripts were then manually referenced to extract and synthesize the core messages from keynote addresses and panel sessions by a single coauthor (GD) with prior training in qualitative methods and thematic coding. Inductive thematic analysis guided the synthesis. Through an iterative coding process, recurring concepts and ideas from field notes and transcripts were identified, grouped, and further refined to derive recommendations. A coding tree is provided in Supplementary Digital Content 1. Only transcript segments relevant to each speaker were shared by email for factual correction.
Additionally, a voluntary, automated post-conference survey was distributed via a convenience sampling strategy. A quick response code was displayed during the closing ceremony, and all attendees were invited to respond. Respondents consented to the use of their anonymous responses for research and conference reporting purposes, and they were blinded to individual researcher identities. Responses were analyzed, and the findings were incorporated into the thematic framework developed from the conference recordings. This mixed-method approach improved validity by incorporating both plenary dialogue and frontline perspectives.
Results
Preconference sessions
PASC opened with hands-on training, at waived or reduced cost, aimed at strengthening the perioperative workforce. Two hundred four trainees from 23 African countries participated in the workshops, which included a microsurgery simulation lab and flap course (N = 28), basic and advanced life support training (N = 45), a pain management series (N = 50), a nontechnical surgical skills workshop (N = 42), and the University of Cape Town Global Surgery Short Course (N = 39). The preconference schedule is detailed in Supplementary Digital Content 2-a.
Main conference
Overview
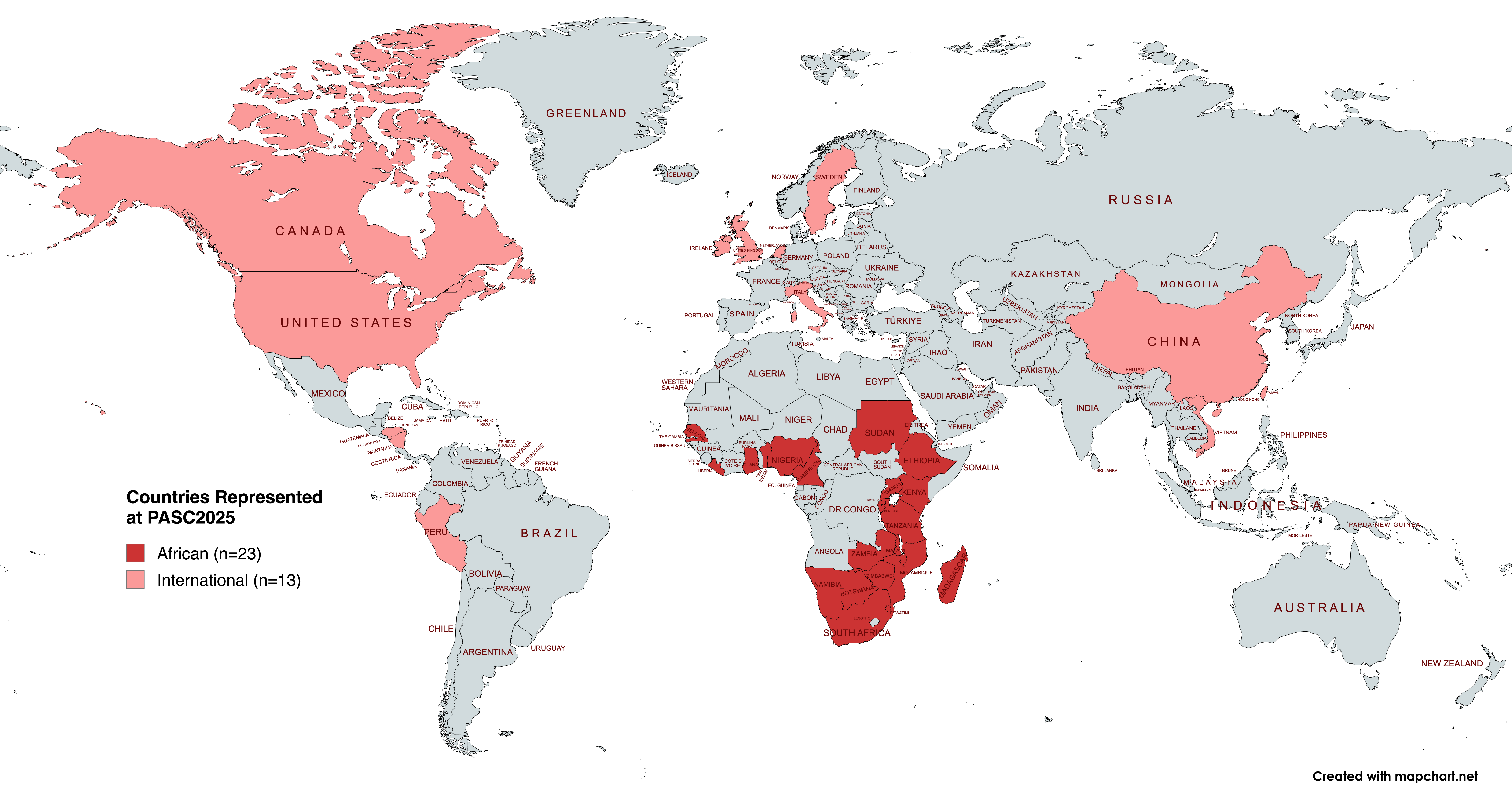
The meeting brought together more than 550 delegates from 36 countries, including representatives from 23 African nations and all sub-Saharan regions (Figure 1). Daily keynote lectures and panel discussions were followed by evening events. The detailed schedule and speaker rosters are presented in Supplementary Digital Content 2 (b-f).

Summarized proceedings
Over the course of 5 days of programming, delegates articulated a unified vision for supporting a massive expansion of Africa’s surgical workforce to meet growing population demands. Daily themes are outlined in Table 2. On the first day the College of Surgeons of East, Central, and Southern Africa (COSECSA) model was discussed as an effective regional solution to overcome the lack of specialty services and local training programs,12 and yet the need for additional competency-based and contextually relevant training programs was recognized. District hospitals were proposed as candidate training sites, which would enable creation of structured career pathways and retention of local talent. Following the theme of promoting African surgical self-reliance, the role of external partnerships was explored. Partnerships that serve local needs over donor priorities were cited as most effective. Innovation was introduced as a key instrument for health systems, and examples of technology and procedural innovations were shared to demonstrate how they improve access, delivery, and safety of surgical interventions.
The lack of visibility for surgery in broader health agendas was identified as a key barrier to workforce expansion, and leadership was called on to elevate surgery in public health discourse. Pathways to increase the representation of surgical voices in policy discussion through leadership and advocacy training were proposed. Evidence from African researchers was presented to support both the need for and feasibility of scaling up the surgical workforce. The subsequent research agenda highlighted the role of data in improving surgical outcomes and advancing global health priorities.13–17 The meeting’s scientific program featured 59 oral abstracts (20 Education, 19 Global Health, 20 Plastic Surgery) and 54 posters, with 78.9% of submissions led by investigators from 15 African countries.
The meeting concluded with sessions on policy and sustainable financing. National Surgical, Obstetric, and Anesthesia Plans (NSOAPs) were discussed as policy frameworks that inform the expansion of surgiccal services, yet implementation barriers, financing constraints, and poor integration with broader health plans were discussed as key challenges.7,18 Representatives from 12 African Ministries of Health were in attendance and contributed to policy discussions, which signaled growing political commitment and recognition of the need for stronger, more integrated surgical systems. The following sections explore these concepts in greater detail.
Delegate experiences and takeaways
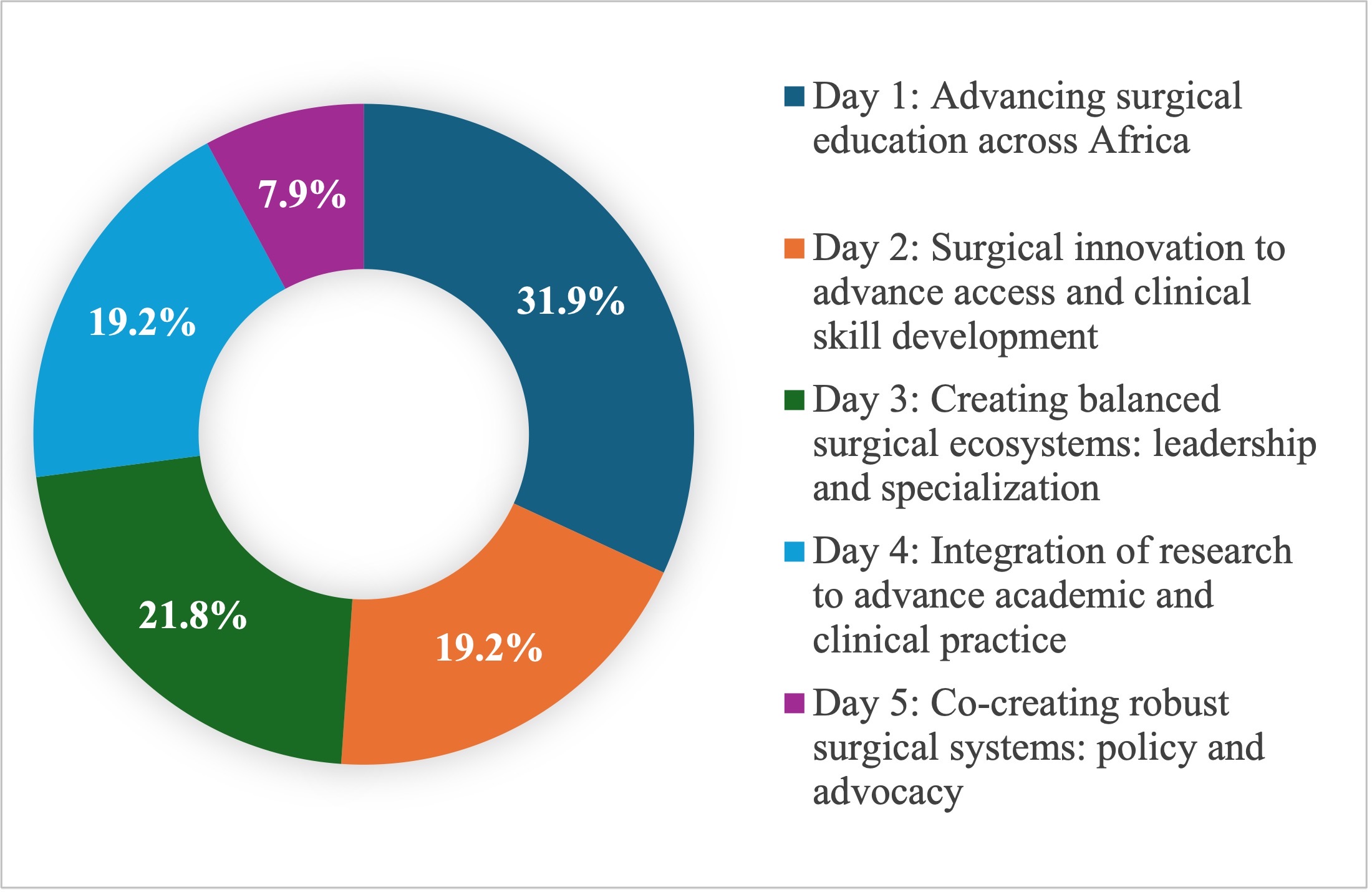
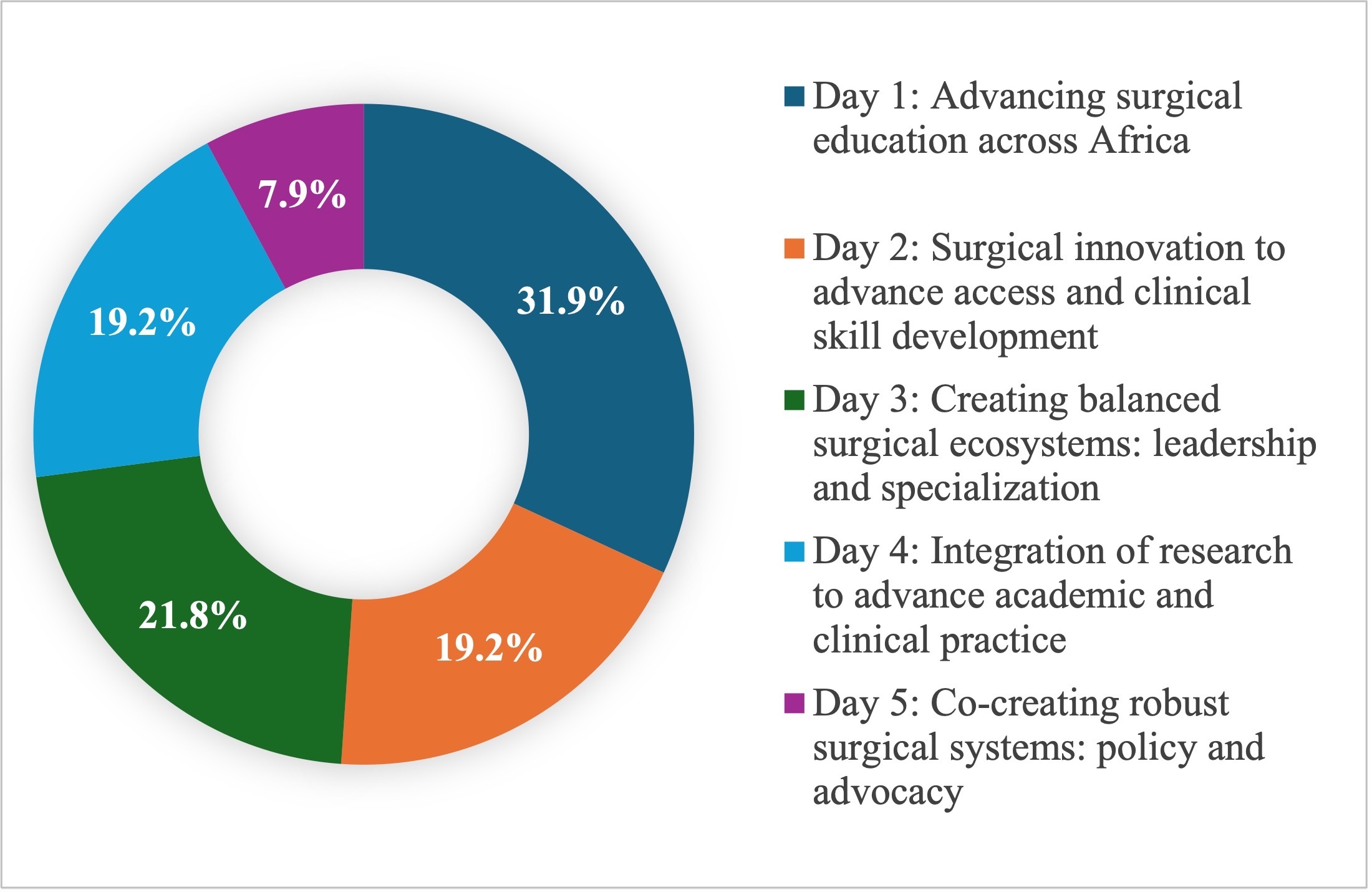
The post meeting survey completion rate was approximately 41% (N = 229 of 558 delegates representing 26 countries). As the survey was distributed on the final day of programming, the number of nonrespondents was unquantifiable as the number of delegates who left the meeting early was unknown. Respondents included surgeons (37%), other medical professionals (31%), residents (14%), students (11%), and nonmedical professionals (6%). Figure 2 shows broad distribution across topics selected as most relevant, though with fewer votes for policy and advocacy. Four recurrent themes were identified from the free-text responses (Box 1) and incorporated into the meeting recommendations.
Key recommendations
Six themes emerged from the meeting content and were translated into recommendations, which are summarized in Box 2 and elaborated in the following sections. These perspectives reflect the real-world, professional experiences of African surgical leaders and multidisciplinary stakeholders who participated in PASC 2025.
Support local clinicians by reinforcing the Pan-African network
The Pan-African Surgical platform was created in response to the recognized need for multisectoral collaboration, which has been the cornerstone of prior successful surgical initiatives. Longstanding partnerships between academic and research institutions, like the Consortium for Advanced Research Training in Africa,19 have increased the quantity and quality of scientific publications from the continent. Similarly, COSECSA’s partnerships between international and regional academic institutions has expanded surgical training across East, Central, and Southern Africa through regional training and knowledge exchange.12 The Strengthening Rwanda Surgery initiative supported Rwanda’s national surgical planning process by engaging experts from regional societies, academia, NGOs, and industry.20 These types of cross-sector collaborations ensure that different perspectives, areas of expertise, and priorities are represented and result in shared ownership of implementation. Therefore, similar coordination between multilateral stakeholders is likely to accelerate the impact and sustainability of solutions for surgical workforce expansion. The Pan-African Surgical and perioperative community created by PASC can serve as a platform for continued knowledge sharing and cross-sector collaboration to achieve this aim.
Expand and enhance the surgical workforce by increasing access to regional training programs
To meet the health care needs of Africa’s growing population, the number of surgeons, anesthesiologists, perioperative nurses, and other health care providers must double by 2030.6 Achievement of this level of growth will require a transition away from costly international fellowships and short-term surgical missions and toward the creation of in-country or regional training hubs. COSECSA’s regional training model eliminates dependency on overseas fellowships, which have been shown to lack appropriate contextual relevance for surgeons returning to Africa. They also can contribute to the loss of surgeons to other countries, known colloquially as brain drain.12,21 Similarly, Rwanda’s South-to-South training collaborative of MOHs, academic centers, the American College of Surgeons, and regional faculty trains surgeons from neighboring countries and reduces reliance on overseas fellowships.22 These models illustrate the success of regional solutions in overcoming training gaps, which is an essential step for expanding workforce capacity. While the need for additional Africa-based training is apparent, complementary pathways that support women’s representation and create leadership pipelines can further strengthen Africa’s workforce.
Promote surgical equity through policy and advocacy
While the WHA68.15 Resolution generated positive momentum for global surgery,1 surgical care remains under-prioritized in national agendas due to inadequate provider engagement, misconceptions about cost-effectiveness, and lack of evidence in many contexts.23 Inclusion of surgery in health policy discourse can increase political support for surgical strengthening initiatives, yet the voices of surgical providers, who understand the challenges faced by local surgical systems, are often lacking in this setting. As Chalwe and Kigera emphasize,24 “The African surgeon is required to do more than provide quality and safe surgical care but to champion surgical systems strengthening outside of the traditional operating room setting.” PASC and the preconference global surgery advocacy course served as entry points for multidisciplinary providers to engage in advocacy roles and promote the global surgery agenda.
Advance context-specific, African-led research
Evidence can guide decision-making, strengthen policies, and reveal inequities in how surgery is delivered to populations. While interest in perioperative research is high among African health providers, significant barriers limit the number of studies that have been produced from the continent.25 Despite the underrepresentation of African-led research in global journals, collaborative initiatives such as the African Surgical Outcomes Study have produced high-impact research that fills critical evidence gaps and informs public health interventions.3 Similar, coordinated efforts between African and global researchers can help reduce barriers to research productivity,15 yet ownership and dissemination of research on African populations by African investigators is key. PASC prioritized African-led submissions for the scientific program and cited mostly Africa-based studies as supporting evidence for this report. Promotion of additional surgical research can be achieved through multidirectional collaboration, engagement of African surgical providers in scientific investigation and peer-review processes, and increased submission to African journals to ensure that findings are disseminated where they are most relevant.
Harness technology and innovation for efficient, equitable care
Quality and access to surgical care are inconsistent across the continent. Technology and innovation can bridge service delivery gaps and should be cautiously embraced by surgical providers. Historically, African facilities have been slow to adopt new health care technologies,26 often viewing them as purely aspirational and nonessential. However, the market for innovation is growing, and the benefits of new surgical technologies are already demonstrated. IRCAD Africa (www.ircad.fr) in Kigali offers minimally invasive surgical platforms that have achieved precision gains, faster recovery, and potential cost reductions, while telehealth and mobile applications have extended training and consultation to previously inaccessible areas.27 As AI and digital tools redefine how health care is delivered around the world, Africa is faced with a decision to adopt contextually relevant innovations or face widening disparities.
Strengthen surgical networks through locally driven and sustainable investments
External solutions applied blindly to African contexts have historically failed. Local solutions for workforce expansion, as presented throughout this report, should be prioritized as they best reflect the unique social, political, and economic realities of African countries.28 In Ghana, local partnerships between teaching hospitals and regional health authorities have expanded surgical access and training in underserved areas with support from national health insurance rather than from external sources.29 Similarly, Tanzania’s NSOAP emphasizes workforce expansion as a priority and incorporated domestic financing to reduce dependency on donations.30 These examples illustrate the feasibility of African self-sufficiency and the importance of prioritizing local and regional solutions over models adapted from dissimilar settings.
Discussion
Many landmark achievements in global surgery have been supported by African leaders, from the Lancet Commission on Global Surgery to the development of national surgical plans.11,31 Despite this backing, Africa remains well below global targets for access and delivery of surgical care. PASC marked a milestone in broader efforts to develop access to safe, timely, and affordable surgical care by achieving multistakeholder engagement and revealing high support for surgical workforce expansion.
Until recently, regional surgical collaborations were limited to academic partnerships and engagement with surgical societies. Surgical societies play an important role in supporting specialty-specific collaboration and increasing research visibility, yet they often operate in siloes. In 2023, PASHeF demonstrated the feasibility of cross-national, whole system planning, and PASC expanded on this model by engaging perspectives from broader stakeholder groups, including patients, private industry, and nonsurgical clinicians. PASC additionally emphasized the inclusion of different linguistic, regional, and gender groups, which are often underrepresented in surgery.15 This design was deliberate as it reflects the ecosystemic nature of surgical systems. Further, the inclusion of differing perspectives added significant value to the discussion. For example, while the need to expand the number of perioperative providers was apparent, delegates emphasized the importance of parallel strategies to support women leaders and encourage policy engagement by the African surgical workforce. By highlighting local expertise and lived professional experiences, PASC discourse contextualized global surgery priorities for Africa’s unique needs and realities.
Finally, the six recommendations produced from the meeting clarified local priorities for scaling up the surgical workforce. Participants shared evidence-based strategies to augment Africa’s surgical teams through national surgical planning, technology and innovation, sustainable health financing, and knowledge exchange. Future adoption of these recommendations into consensus-backed resolutions will enhance the impact of the Pan-African Surgical platform by establishing specific targets and defining metrics for monitoring progress.
Limitations
While PASC included stakeholders from multiple sub-Saharan regions, genders, and professional backgrounds, there was an overrepresentation of attendees from West and East Africa. Selection bias may have contributed to this imbalance, as participation was voluntary and travel costs or clinical obligations may have been prohibitive for those traveling greater distances. Kirengo et al. demonstrated a similar underrepresentation of Southern Africa and Central Africa in collaborative scientific publications,15 which may reflect disproportionate barriers in these regions. Potential strategies to ensure balanced representation in future academic and policy meetings include minimum attendance quotas and funding support. Additionally, the recommendations generated from the conference do not include specific, measurable targets and therefore lack mechanisms for accountability. Future PASC forums will emphasize a formal consensus process to establish actionable and measurable targets for surgical capacity expansion.
Conclusion
PASC engaged leaders from multisectoral backgrounds and across all sub-Saharan regions, demonstrating the feasibility of cross-continental collaboration. The meeting produced 6 recommendations that span training, policy, innovation, and financing domains related to surgical workforce expansion. A future consensus process to ratify these conclusions and establish actionable targets will support continued, measurable progress.
Acknowledgments
We recognize the outstanding contributions of the conference planning committee and supporting organizations, without whose generosity and collaboration this conference would not have succeeded; keynote speakers and panelists, whose expertise and tangible dedication created a welcome space for ideation and collaboration; and finally, Honorable Ministers of Health and their representatives from Rwanda, Ethiopia, Ghana, Kenya, Madagascar, Malawi, Mozambique, Namibia, Seychelles, Tanzania, Zambia, and Zimbabwe, whose vision and unwavering support signaled hope for continued prioritization of surgical systems in national health agendas.
Ethical Approval
This study met criteria for exemption from Institutional Review Board approval. The analysis was conducted on publicly delivered conference proceedings that did not include protected health information. Survey data were collected voluntarily and anonymously, and no identifiable personal data were recorded.
Informed Consent
Participation in the post-conference survey was voluntary. Respondents were provided with an information sharing statement at the start of the survey and indicated informed consent by proceeding. Individuals whose names and quotations are included in the manuscript provided written consent for attribution.
Data Availability
The data underlying this study consist of conference proceedings and anonymized survey responses. Due to the nature of the data collection and absence of a structured dataset beyond what is presented, no additional data are available for sharing.
Conflict of Interest
Several listed authors are salaried employees of Operation Smile Inc.
Funding
Operation Smile Inc. provided financial and logistical support for the Inaugural PASC. It additionally provided funding to affiliated authors for travel, accommodation and registration to attend the conference. The authors received no additional sources of funding for this study.
Use of AI Statement
The use of artificial intelligence (AI) in compliance with TITAN Guidelines (2025) to generate transcriptions from conference audio recordings is detailed in the Methods section. Grammarly (Grammarly, Premium Plan, Version 14.7, 2024) was used exclusively to identify language and grammatical errors. The authors affirm that the use of AI was confined to these purposes and did not influence study design, scientific interpretation, analysis, or conclusions. The authors accept responsibility for the integrity of the content affected through use of AI. The authors declare no conflicts of interest or financial relationships related to Grammarly, Otter.ai, or other AI vendors.