_benefits_of_working_with_visiting_trainees_and_faculty_from_high-income_countries.tiff)
_challenges_of_working_with_visiting_trainees_and_faculty_from_high-income_countries.tiff)
Introduction
Global surgery is a multidisciplinary and intersectoral field that aims to promote equitable access to safe, timely, and affordable surgical care.1 Surgical conditions account for approximately 30% of the global burden of disease, yet 5 billion people worldwide lack access to surgical and anesthesia care.2,3 The past decade saw increased recognition of global surgery and anesthesia priorities within the broader global health agenda, with an emphasis on local needs assessments, capacity-building and infrastructure development, and horizontal health systems strengthening.1,3 Concomitantly, more surgical trainees are expressing a desire to participate in international surgery experiences with up to 71% of US general surgery residency applicants indicating that they would rank a residency program higher if it had a funded global surgery program.4,5
In response to this growing interest and augmented by training accreditation policy changes in high-income countries (HICs), there has been a surge of trainees and faculty from HICs traveling abroad for short-term global surgery engagements, usually in low- and middle-income countries (LMICs).6–9 A 2016 assessment of global surgery experiences by US trainees determined that 34% of US general surgery residency programs offer some form of international experience for their residents.8 While subsequent attempts to quantify current global surgery offerings have been limited by a lack of data on program websites and low response rates, it is evident that interest in global surgery experiences is increasing among HIC surgical trainees.9,10 Recently approved changes to US general surgery program accreditation requirements now mandate clinical experiences in “resource-limited environments” (including LMICs), which may further bolster development of international clinical rotations for surgical trainees from HICs.11
Global surgery rotations for HIC-trainees traveling to LMICs offer multiple benefits including experience working in a cross-cultural setting, exposure to diseases infrequently encountered in high-resource settings, increased autonomy for residents, and exposure to a different system of health care delivery.12–14 However, critics of these unidirectional programs cite concerns that such short-term global engagements are neocolonialist, self-serving, and contribute to continued power imbalances between HICs and LMICs.15,16 Furthermore, the literature is skewed toward studies that report on the benefits to HIC trainees, while few studies have evaluated the perspective of LMIC institutions who host these short-term visitors.17–22 The experience of host institutions is a vital perspective as the globalization of medical education and practice continues.23
To address this gap, our team previously conducted a qualitative analysis of the impact of unidirectional global surgery experiences from the perspectives of surgical faculty and trainees affiliated with a single College of Surgeons of East, Central and Southern Africa (COSECSA)-accredited surgery training program at a tertiary referral hospital in Kijabe, Kenya.22 Several host-perceived benefits and challenges of visitor involvement were identified along with concerns about the lack of a balanced exchange between HIC and LMIC centers and high levels of interest in bidirectional trainee exchange programs. This follow-up study aimed to leverage these findings to more broadly assess the impact of unidirectional visitor involvement from the perspectives of host surgical personnel across all COSECSA-accredited surgical training programs.
Methods
Study Design and Population
Using a staged exploratory sequential mixed methods design, a 56-item survey (see the Supplementary Materials) was developed based on a preliminary, single-institution qualitative analysis.22 In addition to collecting respondent demographics, the survey was designed to assess respondents’ agreement with previously identified perceived benefits and challenges of working with visiting surgical faculty and/or trainees from HICs using 5-point Likert-type questions. The survey also assessed interest in the pursuit of training experiences outside of trainees’ home countries, particularly in HICs, and barriers to bidirectional exchange programs.
All surgical trainees actively enrolled in a COSECSA-accredited program were eligible to complete this voluntary online survey; recent COSECSA graduates within 1 year of completing their program were also eligible to participate. COSECSA is the professional body that fosters postgraduate surgical education and offers surgical training in 14 countries within Central, Eastern and Southern Africa. As the largest surgical training institution in sub-Saharan Africa (SSA), COSECSA administers standardized surgical training programs with a common examination resulting in internationally recognized surgical qualifications for COSECSA graduates. Several COSECSA training programs are affiliated with partner organizations such as the Pan-African Academy of Christian Surgeons (PAACS). PAACS is a US-based service organization that sponsors over 20 surgical training programs at missionary hospitals with a similar geographic distribution to COSECSA. Given that the PAACS sponsorship likely increases exposure to foreign surgical faculty, electives, and institutions and would likely influence survey responses, we also collected information about partner organizations and institutions of respondent training programs.
Data Collection and Analysis
The anonymous online survey was distributed via email through the COSECSA secretariat over a 6-week period from June through July 2022. Given low initial response rates, a senior member of our research team engaged program directors in person at the December 2022 COSECSA Annual General Meeting to provide information about the study and encourage participation. The survey was then redistributed from February to April 2023 over an 8-week period with weekly reminders during this second interval. Survey responses were collected and stored in a secure, web-based Research Electronic Data Capture (REDCap) database.24,25 Responses were summarized using descriptive statistics, namely frequencies and percentages for categorical data. Percentages were calculated based on the number of respondents who completed each question. Statistical analyses were performed with Microsoft Excel Version 16.79.2. Qualitative content analysis was used to analyze the free-text responses.
Ethical Considerations
This study was approved by the AIC Kijabe Hospital Institutional Scientific and Ethical Review Committee (ISERC# KH/IERC/02178/0050/2019), the COSESCA Institutional Review Board (COSECSA/IRB/2022/04), and the Vanderbilt University Medical Center Institutional Review Board (IRB) (IRB# 211079). It adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.26 Informed consent was obtained electronically prior to survey completion.
Results
Participant Demographics and Surgical Training
Of the 990 eligible COSECSA trainees, 223 (22.5%) completed an online survey between June 2022 and April 2023. Most respondents were aged 30–34 years (99, 44.4%) and identified as male (178, 79.8%), married (145, 69.5%), and Christian (187, 83.9%) (Table 1). The most common language spoken by respondents was English (185, 83.0%) followed by indigenous languages (82, 36.8%) and Swahili (57, 25.6%). Respondents identified 23 different home countries (Supplementary Figure A), most commonly Kenya (65, 29.1%), Uganda (29, 13.0%), and Zambia (25, 11.2%).
Nearly all respondents (213, 96%) were surgical trainees while 9 (4.0%) were recent graduates at the time of the survey completion (Table 2). Respondents were most commonly in their first year of training (65, 29.1%), with all remaining years of residency and fellowship training also represented (Table 2). General surgery (115, 51.6%) was the commonest specialty, followed by orthopedic surgery (45, 20.2%), pediatric surgery (26, 11.7%), plastic surgery (17, 7.6%), neurosurgery (9, 4.0%), urology (4, 1.8%), and otolaryngology (4, 1.8%). Most respondents were from training programs in Eastern Africa (200, 89.7%), most commonly in Kenya (71, 31.8%) and Uganda (29, 13.0%) (Figure 1). A quarter of respondents (56, 25.1%) indicated that their training programs were sponsored by PAACS.
Experiences with Visitors
Just over half of the respondents (123, 55.2%) indicated that they have worked with at least 1 visiting trainee or faculty from high-resource countries at their surgical training program, and 41 respondents (18.4%) reported having worked with 5 or more in the last 12 months. Visitors included faculty/consultants (121, 54.3.5%), residents (58, 26%), and fellows (46, 20.6%), who were most often from the US (103, 46.2%) or UK (45, 20.2%).
Benefits of Working with Visitors
Among the respondents who completed the benefits section of the survey (N = 149–153), most agreed that visitors broadened their perspective of how medicine and surgery are practiced in high-resource settings (140, 94.0%), represented a learning opportunity (141, 93.4%), and positively influenced their surgical (131, 86.8%) and clinical (130, 86.1%) skills (Figure 2a). Many also agreed that visitors offered opportunities for networking (128, 84.8%) and mentorship (118, 77.6%), improved the quality of care for local patients (121, 81.2%), positively influenced the prestige and reputation of the local training hospital (119, 78.3%), and gave respondents a sense of validation about their surgical training (117, 77.5%). Fewer respondents agreed that visitors increased their access to resources (106, 70.2%), provided faculty coverage (95, 62.5%), or positively influenced their time management (98, 64.1%) or research skills (92, 61.7%). Additional themes related to the benefits of working with visitors expressed in free-text responses included collaborative learning with the exchange of medical knowledge and skills, exposure to advanced surgical cases and technology, social connection and friendships, research collaborations and institutional partnerships, and reinforcement of evidence-based medicine principles (Table 3).
_benefits_of_working_with_visiting_trainees_and_faculty_from_high-income_countries.tiff)
Challenges of Working with Visitors
Among respondents who completed the challenges section of the survey (N = 148–152), many respondents agreed that short lengths of stay posed challenges when working with visitors (120, 78.9%) and exchange programs between surgical trainees from high-resource countries and low-resource countries is unbalanced (94, 62.7%). Several respondents also agreed that helping HIC visitors adapt and integrate into the local health care system (67, 45.3%), cultural differences (63, 42.0%), and language barriers (58, 38.4%) posed challenges. Approximately a quarter of respondents (38, 25.4%) agreed that power imbalances between high-resource and low-resource countries made it difficult to voice concerns when experiencing challenges working with visiting surgical faculty and/or trainees. Few respondents encountered visitors who were aggressive or confrontational (36, 23.8%) or who demonstrated problematic or unethical behaviors (23, 15.1%), and even fewer (26, 17.3%) felt that their operative experiences were reduced when visiting surgical trainees from high-resource countries were present (Figure 2b). Additional themes related to the challenges of working with visitors expressed in free-text responses included differences in health systems and resource availability, a lack of contextual awareness and adaptability among visitors, and visitor superiority bias (Table 3).
_challenges_of_working_with_visiting_trainees_and_faculty_from_high-income_countries.tiff)
Bidirectional Exchange Opportunities and Barriers
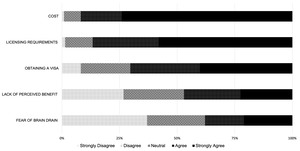
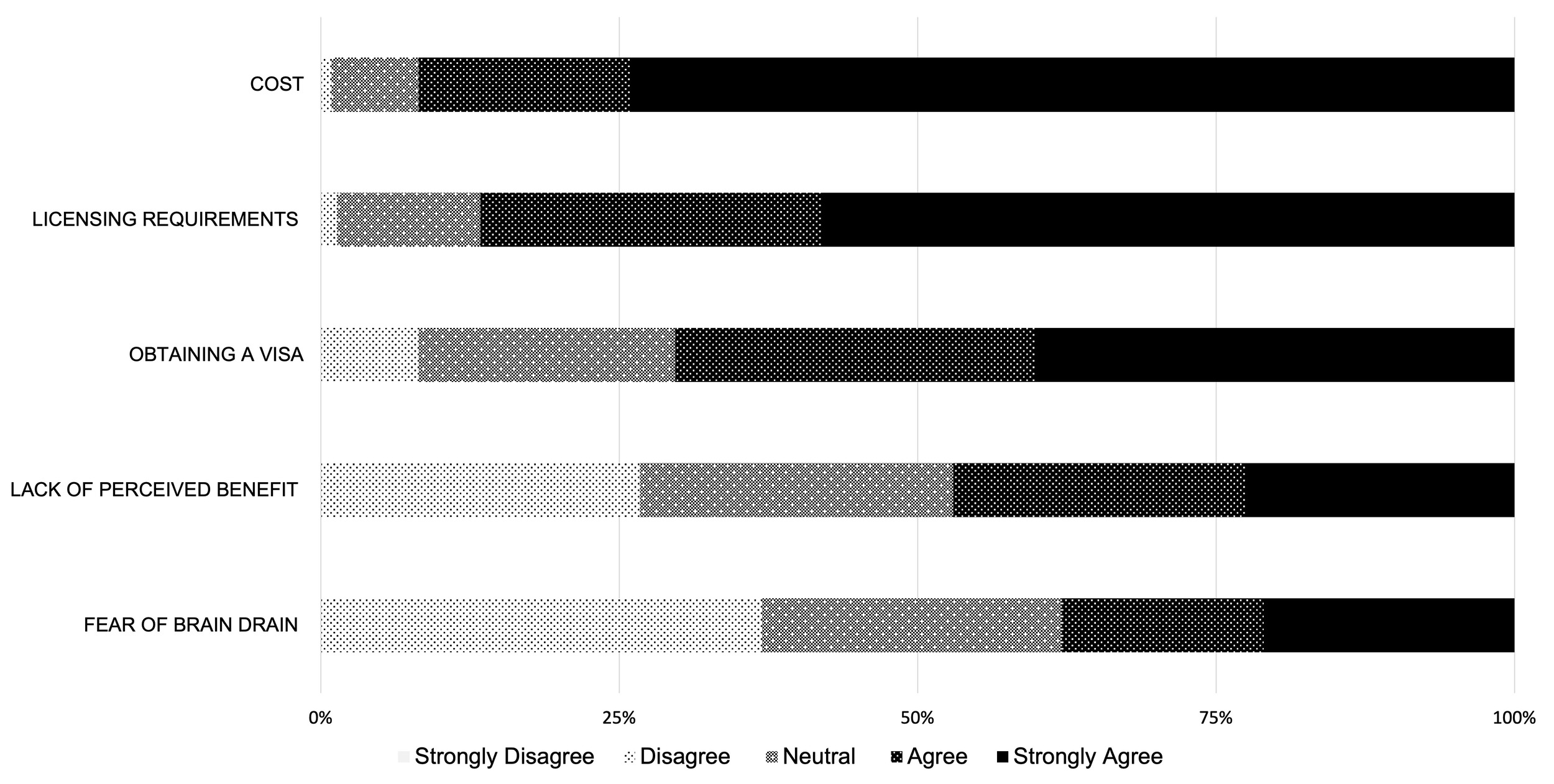
Of the 223 respondents, 63 (28.2%) had participated in a surgical experience outside their home country, but fewer respondents (27, 12.1%) had traveled outside of Africa for that experience and only 20 (9.0%) traveled to a high-resource country. Many respondents desired an opportunity to travel to a HIC for clinical rotations (203, 91.0%) or research fellowships (157, 70.4%). Most (148, 66.3%) would still be interested even if the experience was limited to an observership where they could not scrub into cases or be actively involved in patient care but could participate in research, grand rounds, and other didactic sessions. However, nearly half of respondents (102, 47.0%) agreed that the lack of perceived benefit was a barrier to bidirectional exchange. Other perceived barriers to bidirectional educational exchanges included significant financial and administrative burdens including cost (202, 91.8%), complexity of licensure requirements and paperwork (188, 86.6%), and challenges of obtaining a visa (154, 70.3%). When asked if fear of brain drain posed a barrier to bidirectional educational exchanges, fewer than half (83, 37.9%) agreed (Figure 3). Many respondents expressed in free-text responses that returning to their home country to work was a priority for them because of lifestyle, cultural, and family reasons, which decreases the likelihood of brain drain following training opportunities in high-resource settings. Additional themes related to barriers to bidirectional exchange expressed in free-text responses included lack of existing exchange opportunities, lack of mentorship, lack of financial sponsorship, opposition from local faculty, perceived discrimination from HICs resulting in unequal exchange opportunities, language barriers, and personal/family obligations (Table 4).
Discussion
This international, multi-institutional survey of COSECSA trainees revealed that although visiting surgical faculty and trainees have many positive influences on host trainees, short lengths of stay that require frequent visitor accommodations and integration, unbalanced exchange programs, and language barriers posed challenges. Cultural and health systems differences, visitor superiority complex, and an unwillingness to adapt to local contexts also created conflict. These problems must be addressed to maximize learning opportunities for host trainees. There was an overwhelming desire for collaboration, equitable reciprocity, and bidirectional exchange among the survey respondents. Surgical trainees from LMICs are markedly less likely to participate in international surgery experiences than surgical trainees from HICs. Less than 10% of respondents had prior opportunities to travel to HICs for surgical training, although over 40% had experience working with visitors from HICs and over 90% were interested in traveling to HICs for clinical rotations. Overcoming financial and administrative barriers such as complex medical licensure and visa requirements will be essential for creating reciprocal learning opportunities for trainees from LMICs. Understanding trainee learning goals, aligning exchange objectives with local program priorities, and establishing mentorship and sponsorship pathways will be critical for the success and sustainability of these types of exchange programs.
The benefits and challenges of working with visitors from HICs in our study were similar to those reported in previous studies. A 2022 systematic review of LMIC perceptions of visiting surgical teams from HICs found that the most commonly reported advantages included provision of clinical care, improvement of local skills, health systems strengthening, career benefits, and opportunities for collaboration.20 The disadvantages identified by this review included poor quality of care, lack of follow-up, insufficient knowledge transfer, ethical dilemmas, inequity, competition, language barriers, and administrative and financial issues.20 Notably, these disadvantages reflect the fact that most of the studies in this review assessed visiting surgical teams (e.g., surgical boot camps or mission trips) as opposed to visiting trainees.20 A survey of Ugandan surgical trainees detailing their perspectives toward international collaborators found that most agreed that visitors improved their training through skills workshops and specialist camps; however, nearly half of the respondents felt that the visiting groups had a neutral or negative impact on patient care.17 A 2020 review of international resident rotations, which included 4 studies from LMIC host perspectives, highlighted the potential harms that can result from incongruities between HIC and LMIC expectations and priorities.18 This review found that LMIC trainees appreciated when (1) competition with HIC trainees for surgical cases was minimized, (2) LMIC internal authority was not undermined by HIC trainees, (3) HIC initiatives address local LMIC needs, and (4) LMIC partners were included as authors on research collaborations.18 Our study aligns with and adds to these previous studies by reporting perceptions of a large, diverse cohort of surgical trainees from LMICs. In addition to reporting levels of agreement with previously identified benefits and challenges, respondents were given the opportunity to voice additional perspectives through free-text responses, which revealed the importance of bilateral exchange, a desire for lasting social connections, and the need for understanding and adapting health care delivery to local contexts.
Beyond the benefits and challenges of existing unidirectional international surgery opportunities for HIC trainees, our findings demonstrate a resounding demand for reciprocal opportunities for LMIC trainees. Global health leaders have long emphasized the need for reciprocity and bidirectional exchange between HICs and LMICs, and global surgery programs must follow suit.14,23,27,28 Our study revealed several financial and administrative barriers to equitable exchange including travel-related expenses (e.g., flights, accommodations, and visa fees), rotation-related expenses (e.g., qualifying examination and licensure fees, malpractice insurance, drug testing, and background checks), and health-related expenses (e.g., mandatory vaccinations).28 The limited accessibility of prerequisite requirements in LMICs (e.g., access to testing centers or vaccinations) exacerbate these hurdles.
Interestingly, trainees expressed that their local program leaders, administrators, and governments often opposed international learning opportunities in high-resource settings. This may be explained by the high costs, logistical hurdles, or lapses in local coverage while trainees are abroad. Fear of health worker migration, or “brain drain”, may also influence opposition to international educational exchange opportunities, particularly within programs where the mission is to train surgeons who will remain in LMICs. Further evaluation of perceptions about international educational exchange programs in HICs and assessment of LMIC trainee goals for international experiences can help garner the top-down support necessary for successful collaboration.
Limitations
This study is limited by its low response rate (22.5%), which could indicate an underlying sampling bias or non-response bias. Our study sample demonstrated overrepresentation of Kenyan trainees, and most of the trainees in this study were male, junior level, and from general surgery programs. The survey was also only distributed in English, which limited responses from trainees from programs where English is not the primary language. Thus, the results may not represent the views of our target study population. Future studies assessing perspectives of underrepresented groups would help address this response bias.
Despite these limitations, this is one of the largest studies to date of LMIC surgical trainee perspectives with programs from 18 different countries and 8 different surgical specialties represented. Further assessment of host perspectives and needs with intentional, multipronged dissemination of these findings to key stakeholders, including policymakers and leaders in surgical education, will be critical for achieving equitable global surgical education partnerships with reciprocal opportunities for LMIC trainees.23,29
Conclusion
Short-term global surgery engagements provide important benefits to local trainees and health care systems but also pose challenges that warrant mitigation. Additionally, there remain numerous barriers to reciprocal clinical education opportunities for LMIC health care personnel in high-resource settings despite a strong expressed desire for these educational opportunities from practitioners in LMICs. Ongoing advocacy is essential for promoting equity in global surgery training through more balanced, bidirectional engagement. These efforts will not only improve trust and foster a sense of mutual benefit, but they will also enhance the sustainability of global partnerships.
Recommendations
Bidirectional exchange opportunities that benefit trainees from HICs and LMICs should become more widely available. They should be intentionally designed to address the learning objectives of both LMIC and HIC trainees and should include structured onboarding with cultural integration training. Policy changes such as temporary medical licensure and the creation of special visa categories can lessen the logistical burdens placed on foreign learners and can increase their potential for meaningful clinical engagements beyond observerships.14 An example of successful legislation change is the passage of the Tennessee “Visiting Fellows Act” in 2022, which created a short-term license for clinical medical education of foreign medical graduates with stipulations related to supervision, malpractice coverage, and rotation duration.30,31 The American College of Surgeons Coalition for Building Reciprocal Initiatives for Global Health Training is also garnering support for J-1 visa amendments to promote equitable access to surgical training opportunities for trainees from LMICs.32
Increasing equity in global surgery training will strengthen international partnerships, enhance clinical and surgical capacity, and ultimately result in improved health outcomes globally.
Acknowledgments
The authors wish to acknowledge all individuals from COSECSA who helped distribute and/or completed this survey. We would also like to thank the AIC Kijabe Hospital Department of Surgery and Vanderbilt University Medical Center Section of Surgical Sciences for their support of this project.
Ethical Approval
This study was approved by the AIC Kijabe Hospital Institutional Scientific and Ethical Review Committee (ISERC# KH/IERC/02178/0050/2019), the COSESCA Institutional Review Board (COSECSA/IRB/2022/04), and the Vanderbilt University Medical Center Institutional Review Board (IRB) (IRB# 211079).
Informed Consent
Informed consent was obtained electronically prior to survey completion.
Data Availability
Deidentified datasets generated and analyzed in this study are available from the corresponding author upon reasonable request.
Conflict of Interest
Laston Chikoya is the current president of COSECSA. Chelsea Shikuku received the COSECSA-Intuitive Foundation Travel award at the 24th COSECSA Annual conference, in December 2025 based on the findings of this study: This award supported travel expenses, visa fees and conference fees, meals, and accommodation. Shikuku is also an unpaid member of the Kijabe Hospital Institutional Scientific and Ethics Review Committee beginning in November 2024, however she was not involved in the ethics review for this study. Rondi M. Kauffman attended the American College of Surgeon Advocacy Summit with travel costs paid by the American College of Surgeons. Kauffman is also an ECAJS Editorial Board Member, Vice Chair of ACS H.O.P.E. Advocacy Committee at the American College of Surgeons, and Chair of Global Surgery Taskforce through the Association of Program Directors in Surgery.
Funding
Please note that Catherine N. Zivanov received funding from the Washington University School of Medicine Surgical Oncology Basic Science and Translational Research Training Program Grant T32 CA009621 from the NCI during Academic Year 2023-2024. Zivanov also received funding during Academic Year 2024–2025 from the Memorial Sloan Kettering Cancer Center Stern Fund to support professional development during general surgery residency, during which time this manuscript was prepared. Zivanov received funding during Academic Year 2019–2020 to conduct the pilot qualitative study that led to the development of this survey.
Rondi M. Kauffmann received the NIH NCI breast cancer research grant with payment made to their institution. They also received Wellcome LEAP grant for laparoscopy training with payment made to their institution and received honoraria for giving surgical grand rounds at Wayne State University and Medical College of Wisconsin.