Introduction
Musculoskeletal injuries are among the major contributors to the global disease burden, affecting 20–50 million people worldwide each year, preventing patients from normal societal interactions and from working to meet their financial obligations.1 Most of these injuries result from motor traffic crashes and lead to significant morbidity and mortality, especially among the young population in low- and middle-income countries like Tanzania. Due to high-velocity impact and a limited soft tissue envelope, most of these patients sustain open tibia fractures with various complications.2–4
These patients may experience anxiety and fear related to the injury, the healing process, and potential complications, including uncertainty about recovery outcome, pain levels, and the need for long-term rehabilitation.5 Body image concerns may arise from the visibility of the open wound and from the use of immobilization devices, causing self-consciousness, embarrassment, and a negative body image.6 Delays in recovery might affect the survivors’ mental health, which may lead to the development of psychological distress following the trauma.7,8 Generally, the global proportion of psychological distress in orthopaedic trauma patients is stated to be 3–5 times higher than in the general population.9 Patients in developing countries are more likely to experience psychological distress when compared to those in the developed world.8,10 Despite the presence of psychosocial morbidity in patients with open tibia fractures, clinical assessment of psychological distress during pain management treatment may improve patients’ clinical outcomes during post-injury care.11
This study aimed to assess the rate of psychological distress and the associated factors among patients with open tibia fractures treated at Muhimbili Orthopaedic Institute (MOI).
Methodology
Study design and area
A hospital-based cross-sectional study was conducted at MOI in Tanzania. Patients requiring mental or psychological evaluation at MOI are normally attended by experts from the department of Psychiatry and Mental Health of Muhimbili National Hospital (MNH), located within the same compound, upon consultation.
Inclusion and exclusion criteria
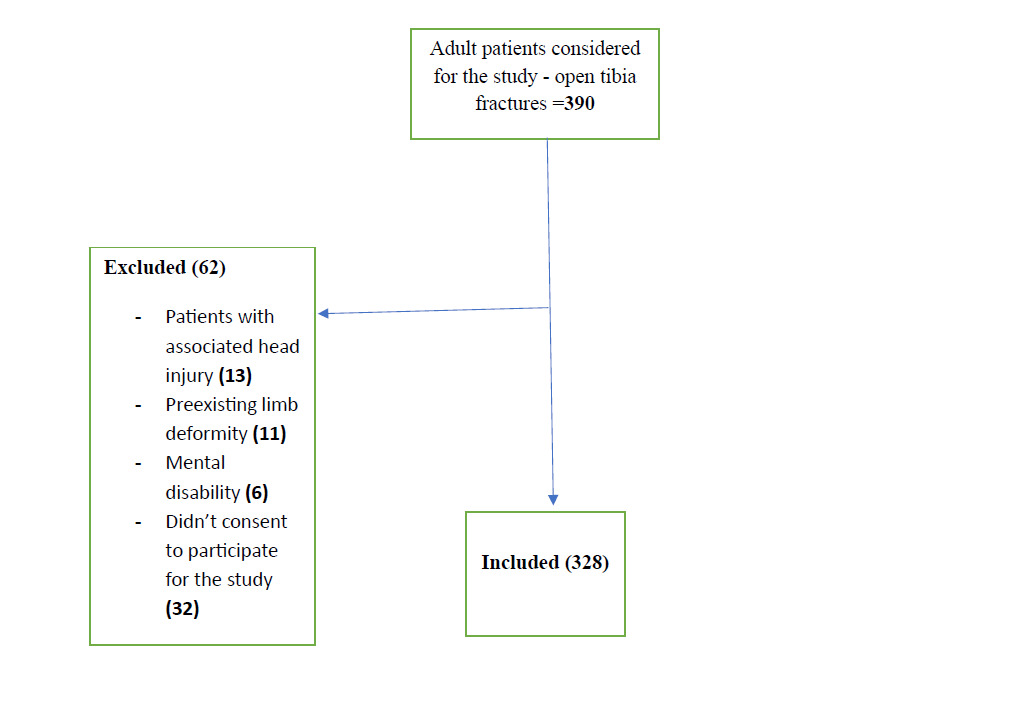
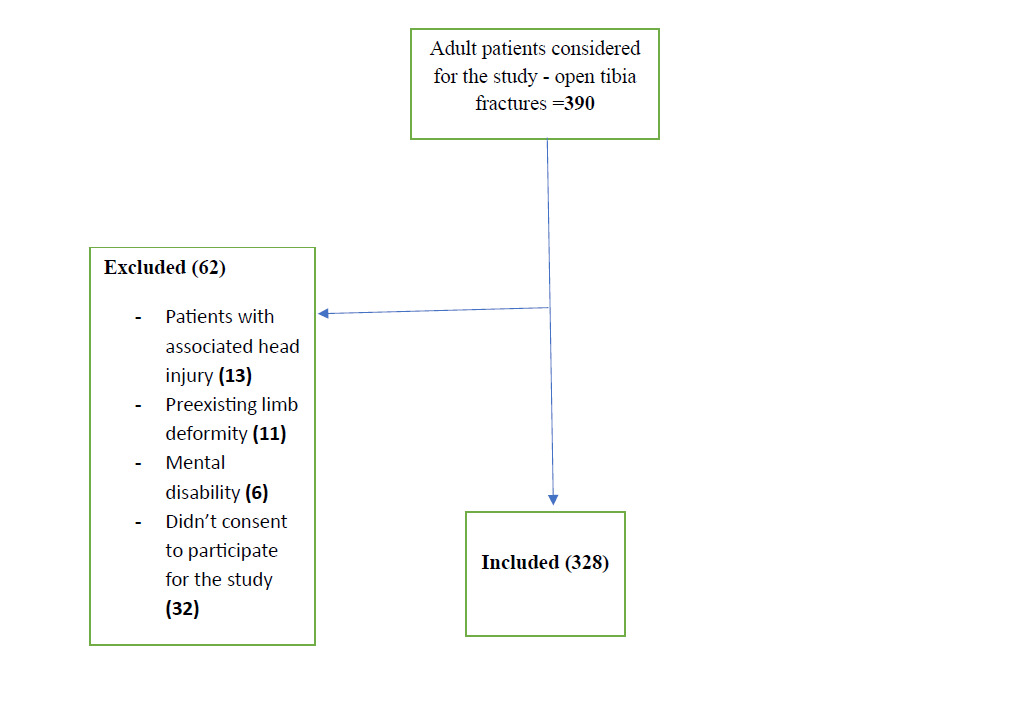
We included all patients with an open tibia fracture aged 18 years and above, excluding those with preexisting limb deformity, pathological fractures, cognitive impairment (such as head injury, stroke, and dementia), or with established psychiatric diagnoses (such as schizophrenia, and major depressive disorder).
Study variables
The dependent variable was psychological distress. The short form 36 questions (SF-36) with mental health (MH) scores were used to assess quality of life, focusing on mental health functioning levels.12,13 Due to the absence of established normative data of the Tanzanian population on SF-36 scores, a 60% threshold was adopted from the quality-of-life study conducted at MOI, which identified 60% as the baseline for good mental functioning. Therefore, those who scored below that on the mental health domain in our study were categorized as indicative of psychological distress.14
Independent variables included sociodemographic characteristics and trauma-related factors such as mechanism of injury, fracture classification, length of hospital stays, payment mode, and treatment provided.
Data collection procedure
A consecutive sampling technique was used to recruit the study participants at the inpatient or outpatient departments after obtaining their informed consent, where data were collected using a structured questionnaire in face-to-face interviews. To ensure its validity, the questionnaire was reviewed by experts in mental health, epidemiology, and biostatistics, followed by a pilot study involving 10% of the sample size (n = 33) before engaging in the actual study. The study’s findings were used to refine the tool.
Data management and analysis
The collected data were analysed by SPSS (Statistical Package for Social Sciences) software version 24 (IBM Corp., Armonk, NY, USA). The variables were summarized by the frequency distribution table, and the description of continuous variables was done using mean and standard deviation. The Chi-square test was used for comparison of categorical variables, whereas the t-test was utilized for continuous variables. A P value of less than 0.05 was regarded as statistically significant. A logistic regression analysis was done to determine the effect of each independent variable. The proportion of patients with psychological distress was calculated as a ratio of those with psychological distress (numerator) to the total number of participants (denominator) in percentage.
The body mass index was assessed by dividing mass (Kg) by height2 (meter2), while pain severity was assessed by the numeric pain rating scale, with 0 being no pain and 10 being the worst possible pain. The social support was assessed by the Oslo Social Support Scale (OSSS-3), where individuals with scores of 3–8 were termed as having poor social support, 9–11 as moderate, and 12–14 as strong10–12
Ethical consideration
Ethical approval was secured from the Muhimbili University Institutional Review Board (Ref: MUHAS-REC-01-2023-1496), and permission to collect data was obtained from MOI. Confidentiality was maintained throughout and after the study. To ensure respondent anonymity, a questionnaire was designed without names or identifiers. Additionally, all participants were informed of the study’s objectives so they could make an informed and voluntary decision about participation. They were also given the right to withdraw from the study at any time without penalty. Consequently, study participants were asked to sign a written consent form before completing the questionnaire. Mental health services were offered for participants with marked psychological distress upon consultation from the expert department at MNH.
Results
We found 390 patients with open fractures, out of which 328 patients were enrolled after providing their informed consent (Figure 1).
Socio-demographic characteristics of patients with an open tibia fracture
The mean age of participants was 35.04 ± 12.61 years, with more than half of them (70.7%) aged 18–38 years. 265 were male, accounting for 80.8% of the total population. One 178 participants had completed secondary education, contributing to more than half of the participants (54.3%). The majority were single (70.1%) and privately or self-employed (81.1%). Most (68.3%) had a monthly income of less than $200 USD and had no health insurance (91.5%) (Table 1).
Trauma-related factors among patients with an open tibia fracture
Most participants (39.0%) were more than 6 weeks post-injury, 33.8% of them had complications, including amputation, delayed union, infection, and non-union. 82.0% reported having pain.
Proportion of patients with psychological distress as a result of an open tibia fracture
Our study found 218 participants to have psychological distress based on their score, amounting to 66.5% of the total population.
Association between psychological distress and demographic characteristics of patients with open tibia fracture
We found a significant association between psychological distress and level of education (P value = 0.026), occupation status (P value = 0.001), monthly income (P value = 0.00), and social support (P value = 0.001). However, there was no significant association with age, BMI, sex, marital status, number of children, or religion (Table 2).
Association between psychological distress and trauma-related factors
There was a significant association between psychological distress and the time since the injury (P value = 0.016), the presence of complications (P value = 0.001), pain severity (P value = 0.003), and the modality of payment of hospital bills (P value = 0.006). However, there was no association with fracture severity, mechanism of injury, or type of surgical treatment received (Table 3). Factors with a P value of 0.2 or less, including education level, occupation status, income status, social support, duration since injury, presence of clinical complication, mode of hospital bill payment, age, marital status, and having children were involved in multivariate analysis. Poor social support (AOR = 4.1, 95% CI:1.171–14.666, P = 0.027), primary education level (AOR = 2.645, 95% CI:1.313–5.331, P = 0.007 ), unemployment (AOR = 2.394, 95% CI: 1.310–4.387, P = 0.006 ), low income (AOR = 2.366, 95% CI:1.286–4.350, P = 0.005), presence of clinical complications (AOR = 3.216, 95% CI:1.745–5.925, P = 0.00 ), acute post-injury phase (less than three weeks; AOR = 3.057, 95% CI: 1.526–6.124, P = 0.002 ), and lack of health insurance (AOR = 4.312, 95% CI:1.450–12.824, P = 0.009) were found to be independent predictors of psychological distress (Table 4).
Discussion
Proportion of psychological distress
The proportion of psychological distress among patients with open tibia fractures from this study was 66.5%, which was higher than the results of a study conducted in Ethiopia that found 35.4% of the orthopaedic trauma patients to have psychological distress.8 These findings suggest that open fracture patients may exhibit a higher level of mental disturbance compared to other orthopaedic conditions, which may be due to wounds that can affect body image perception, increase the need for prolonged care, or increase the risk of developing chronic complications. In the USA, 26% of the trauma patients had psychological distress,15 which is lower than ours. This could be attributed to the differences in patients’ income levels, education levels, and employment status. Most of our patients had a monthly income below the poverty line with limited access to health resources, which might potentially impact their mental health and contribute to a higher proportion of psychological distress.16–18 Furthermore, variations in healthcare infrastructure, mental health awareness, and support systems between the countries may also affect stress management and treatment-seeking behaviours.
Factors associated with psychological distress among patients with an open tibia fracture
The poor quality of life of patients with tibia fractures can be influenced by poor mental health, exacerbated by levels of depression, anxiety, and psychological distress.10,19,20 The following factors are associated with higher levels of psychological distress among patients treated in our setting.
Level of education
We found an association between psychological distress and lower education levels, which may result from limited access to resources and reduced opportunities, such as employment, income, and lack of social support.21 These findings were contrary to the study done in Ethiopia, where the education status was not significantly associated with psychological distress.22 This variation could be explained by the difference in the demographic profile of the study population, where only 13% of our study participants were above high school level, while 29% of the participants in Ethiopia were above it.
Employment status
Unemployed patients were 2.3 times more likely to report developing psychological distress when compared to employed patients. It has been reported that 40.6% of patients with orthopaedic conditions in Tanzania were at risk of depression after losing their jobs as a result of delayed recovery from injury and return to work.23 A similar observation was reported by Becher et al.11 Patients with long bone fractures have limited opportunities due to their incapacity to participate in regular activities,24 whereby the stress of running a business, meeting deadlines, and dealing with financial risks can contribute to higher levels of psychological distress.
Income status
Patients with lower income levels (less than $200 USD per month) were more highly associated with the development of psychological distress than those with higher levels of income above it. Our findings concur with a study done in the USA, which reported that injured patients with financial constraints were strongly related to limited access to rehabilitation services.25 The association between lower income levels and psychological distress could be attributed to socioeconomic inequalities, stigma, and marginalization.26,27 Therefore, psychological distress associated with income disparity could be due to negative emotional feelings impacting mental health, resulting from limited access to healthcare.
Social support
Patients with poor social support were significantly associated with psychological distress compared to patients with good social support, which aligns with the results of other studies done in Ethiopia.22,28 Findings have suggested that, during the healing process, social support can help to provide emotional comfort, practical aid, motivation, information, and a sense of belonging.
Duration since injury
The patients in the acute post-injury phase were 3 times more likely to report psychological distress than those who had older injuries, emphasizing the importance of understanding and addressing the psychological impact during the early stages of recovery from an open tibia fracture. On the contrary, studies conducted in Australia and New Zealand reported that injured patients experienced significant psychological distress during hospitalization and 3–6 months following hospital discharge.29,30 Variation in these findings could be attributed to the difference in sample sizes and geographical location.
Presence of complication
Patients with open tibia fractures who developed complications were more likely to develop psychological distress than those who didn’t, which is consistent with the findings of the study done in Addis Ababa, Ethiopia.22 Furthermore, the study by Ababu et al. in 2022 reported that psychological distress among orthopaedic patients in southern Ethiopia was commonly associated with complications such as depression, post-traumatic stress disorder, and personality disorder.28 This reflects the significance of this factor across countries in sub-Saharan Africa.
Mode of healthcare payment
Participants who were not insured and paid cash for hospital bills were 4.3 times more likely to report psychological distress, according to a systematic review, which reported that the likelihood of psychological distress was significantly associated with a lack of health insurance among patients with open tibia fractures.31 The cost of medical care imposes a significant financial burden, resulting in financial strain associated with worries about medical expenses and severe psychological distress.
Injury severity
There was no significant association between the fracture severity based on Gustilo and Anderson grading and the psychological distress among our study participants, which implies that the psychosocial factors may be more important than the physical injury itself in determining the mental health outcomes.
Conclusion
We found a high proportion of psychological distress among patients with open tibia fractures, regardless of their severity or treatment offered in our setting. This is significantly associated with low education levels, unemployment, lower income, poor social support, the acute post-injury phase, and the presence of complications. Therefore, efforts should be directed to include the mental component of treatment when caring for patients with open fractures based on their risk profile, with more emphasis on psychosocial factors.
Study Limitations
There is a possibility of social desirability bias, where respondents may report what they believe the researcher wants to hear during a face-to-face interview. Furthermore, while the use of 60% cut off point on the SF-36 was adopted from local literature, it has not been formally validated as the diagnostic threshold for psychological distress in Tanzania, calling for cautious interpretation.
Ethical approval
Ethical approval was obtained from the Muhimbili University Institutional Review Board (MUHAS-REC-01-2023-1496).
Informed consent
Written informed consent was obtained before the questionnaire was completed.
Data Availability
The data that support the findings for this study are available from the corresponding author upon reasonable request.
Conflict of Interest
None
Funding
None