Introduction
Thoracic empyema is characterized by the accumulation of purulent exudate within the pleural space, frequently manifesting as a sequela of pneumonia, tuberculosis, or the secondary infection of undrained posttraumatic hemothorax. The pathology progresses through distinct stages; once it reaches the organized phase (stage III), patients face a heightened risk of complications that typically necessitate definitive surgical intervention via open thoracotomy and decortication.1,2 This complex inflammatory condition evolves over approximately 5–6 weeks. Due to its heterogeneous clinical, microbiological, and radiological presentations, establishing a singular standardized classification remains a diagnostic challenge.3–6 Empyema is classified as either primary or secondary, with secondary cases following thoracic trauma or surgical procedures.7–10
In resource-limited settings, delayed clinical presentation, diagnostic inaccuracies, suboptimal management protocols, a high tuberculosis (TB) burden, and restricted access to modern therapeutic modalities remain the main causes of morbidity and mortality.11–13 Globally, the incidence of thoracic empyema is rising, a trend potentially linked to increasing antimicrobial resistance and the significant tuberculosis burden in low- and middle-income countries.14–16 In our clinical setting, tuberculous empyema and trauma-associated empyema represent the most prevalent etiologies of organized thoracic empyema.
Establishing an accurate etiological and stage-specific diagnosis is critical for effective treatment planning and optimizing clinical outcomes.17–22 Diagnosis requires a comprehensive clinical workup, including laboratory investigations, microbiological cultures, radiological imaging, and occasionally histopathological confirmation.23–25 In environments where essential diagnostic infrastructure and specialized clinical experience are limited, patient prognosis is heavily influenced by comorbid status, etiology, disease stage, and the available therapeutic options.26–28 The management of empyema is multimodal, requiring targeted antibiotic therapy specific to the causative pathogen and a determination of the most effective drainage procedures, whether by thoracentesis, tube thoracostomy, video-assisted thoracoscopic surgery (VATS), or open decortication.24,29,30 While the initial strategy is likely determined by disease stage and patient factors, it is often constrained by institutional resources and the available surgical scope of practice.
Hence, in Ethiopia, restricted access to specialized thoracic surgical care frequently results in protracted delays in definitive intervention. These inconsistent care patterns and resource scarcities likely compromise management outcomes; however, there is limited local evidence of thoracic empyema, particularly none within HUCSH. Therefore, this retrospective, single-center study serves as a foundational step for future large-scale multicenter research for better identifying of the independent predicting factors associated with thoracic empyema surgical management outcomes.
Methodology
The study was conducted at Hawassa University Comprehensive Specialized Hospital (HUCSH), situated at 7°3′N and 38°28′E on the eastern shore of Lake Hawassa in Sidama. HUCSH is a tertiary teaching and referral center providing undergraduate and postgraduate medical training while delivering specialized clinical care to a catchment population of approximately 20 million across Sidama, SNNPR, Southern Oromia, and the Somali region, as well as to referrals from Somalia and Kenya. Established in 2003, the hospital operates 450 beds and manages over 102,033 patient visits annually. The thoracic surgery unit, established in 2023, initially focused on core thoracic procedures and postgraduate surgical training. Recently, the unit has expanded to offer advanced minimally invasive thoracic procedures, such as VATS and diagnostic thoracoscopy, and functions as a cardiothoracic surgery research center.
The study employed a retrospective cohort design, conducted over the period from January 1, 2023, to December 31, 2025. All patients with thoracic empyema who underwent surgical management and possessed complete medical records during this time frame were included to maximize the case capture rate. This design was selected to facilitate the assessment of temporal relationships between preoperative risk factors and postoperative clinical outcomes using existing medical records.
Data collection was performed by trained nurses, medical interns, and junior surgical residents. A structured, pretested checklist was utilized to extract relevant clinical data from physical patient charts since the facility does not currently use an electronic medical record system. Medical record numbers were identified through the report logs for emergency medicine, internal medicine, and the surgical department, as well as through the admission logs for thoracic surgery and the operating theatre. Data were entered into the Kobo Toolbox platform, where each checklist was assigned a unique code to ensure accuracy and consistency. The dataset was subsequently exported to SPSS version 26.3 for statistical analysis.
Study variables encompassed sociodemographic characteristics (age, sex, and residence) and comorbidities (diabetes mellitus, hypertension, and HIV/AIDS). Clinical variables included presentation (duration, symptoms, and signs) and the etiology of empyema (post tuberculous, posttraumatic, and parapneumonic complications). Diagnostic imaging modalities including chest X-ray, ultrasound, and CT scan were recorded, alongside surgical interventions (closed tube thoracostomy and open thoracotomy and decortication). Outcome measures included surgical results (favorable vs unfavorable, resolution, and the requirement for reintervention), postoperative complications, length of hospital stay, and in-hospital mortality. After confirming the interdependence of outcome variables via chi-square testing, a primary measure of overall surgical outcome was established, alongside secondary endpoints such as reintervention and complete resolution.
An analytical framework was employed to identify factors influencing overall surgical outcomes, the necessity of reintervention, and complete resolution. Initially, chi-square and Fisher’s exact tests were used to assess associations between potential predictors and both primary and secondary outcomes. In-hospital mortality and postoperative complications were excluded from certain bivariate analyses because they violated chi-square validity assumptions; these are reported descriptively in their respective sections. Confounding variables were identified and addressed through restriction and sensitivity analysis. Variables demonstrating significant or clinically relevant associations in bivariate binary logistic regression were subsequently entered into multivariate binary logistic regression models to identify independent predictors for each outcome.
Operational definitions included:
-
Favorable surgical outcomes were when patients recovered fully following the initial treatment, without surgical reinterventions or in-hospital mortality,
-
Resolution of empyema was defined as complete clinical improvement with radiological clearance of pleural collection following the initial treatment, without evidence of persistent or recurrent disease during the hospital stay and follow-up periods,
-
Reintervention was defined as the requirement for any additional invasive procedure after the initial treatment, including repeat tube thoracostomy or open decortication.
Results
Overview
Over a 3-year study period, a total of 102 patients were identified who met the inclusion criteria, having undergone surgical management of thoracic empyema. Following a review of medical records, 83 patients possessed comprehensive clinical documentation and were included in the final cohort. The remaining 19 cases were excluded from the study due to insufficient records (n = 12) and untraceable medical charts (n = 7).
Sociodemographic characteristics of thoracic empyema patients at HUCSH
The median age was 45 years (IQR, 26–64), with 42% of patients aged 40–64. A male predominance (69.9%) was observed. Most patients originated from the Sidama region (37.3%), and 67.5% were rural residents. Comorbidities were present in 45.8% of the cohort, most commonly HIV/AIDS (13.3%), while 2.8% reported a cigarette smoking history.
Clinical presentation characteristics of thoracic empyema patients at HUCSH
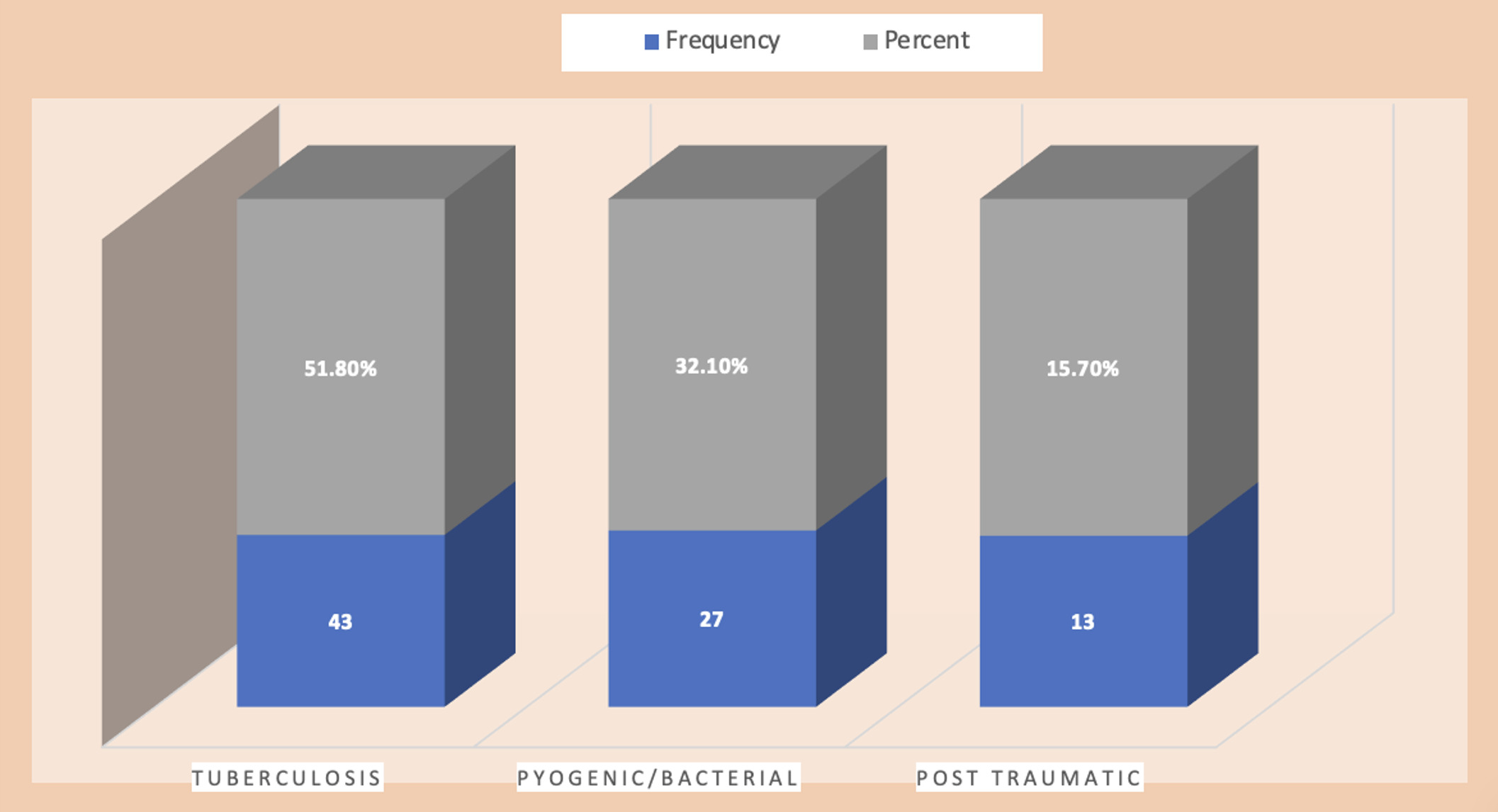
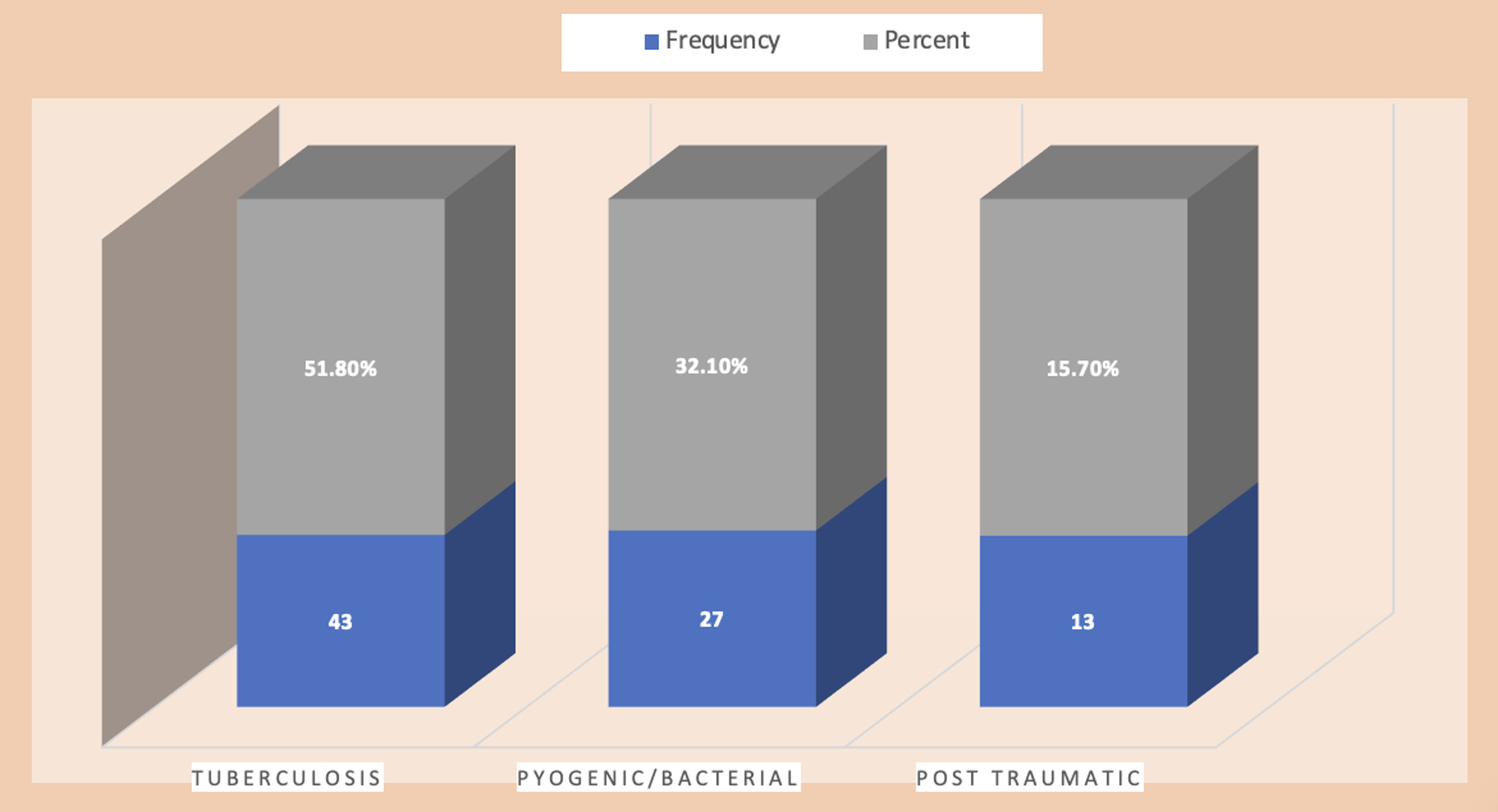
The median symptom duration prior to presentation was 7 weeks (IQR, 5–8). The primary complaints were chest pain and dyspnea. Physical examination frequently revealed dullness to percussion and diminished breath sounds. At admission, 27.7% of patients had a chest tube in situ, while 42.2% reported prior hospitalization, predominantly in medical wards. More than one-half had received antituberculosis therapy or broad-spectrum antibiotics. Right-sided involvement occurred in 50.6% of cases. The leading etiologies were tuberculosis 51.8%, while post trauma was about 15.7% (Figure 1)
Laboratory and radiologic characteristics of thoracic empyema patients at HUCSH
In most patients, complete blood count and various sequences of diagnostic imaging were performed, whereas confirmatory microbiological tests were obtained in about 45.8%. The majority of patients demonstrated elevated white blood cell counts with neutrophil predominance, and Staphylococcus aureus was the most commonly identified bacterium among culture tests. Chest ultrasound was performed for 78.3% of patients, while 69.8% received chest CT scans. The majority (50.6%) of empyema patients were multiloculated in both imaging modalities, and about 39.8% were in the organizing stage (stage III). Among microbiological tests, GeneXpert was the most commonly used confirmatory test for tuberculosis; however, it was positive in only 26.5% tuberculous empyema cases (Table 1).
Preoperative diagnosis and management of thoracic empyema patients at HUCSH
As the only specialized cardiothoracic referral center in the region, we frequently manage patients who present late with missed diagnoses and suboptimal investigations leading to initial medical ward admissions and further significant diagnostic delays. Many patients in our study had already commenced empiric antibiotic or antituberculosis therapy or had undergone tube thoracostomy at peripheral facilities without a definitive diagnosis. Upon evaluation at our center, management was primarily dictated by the disease stage and clinical status.
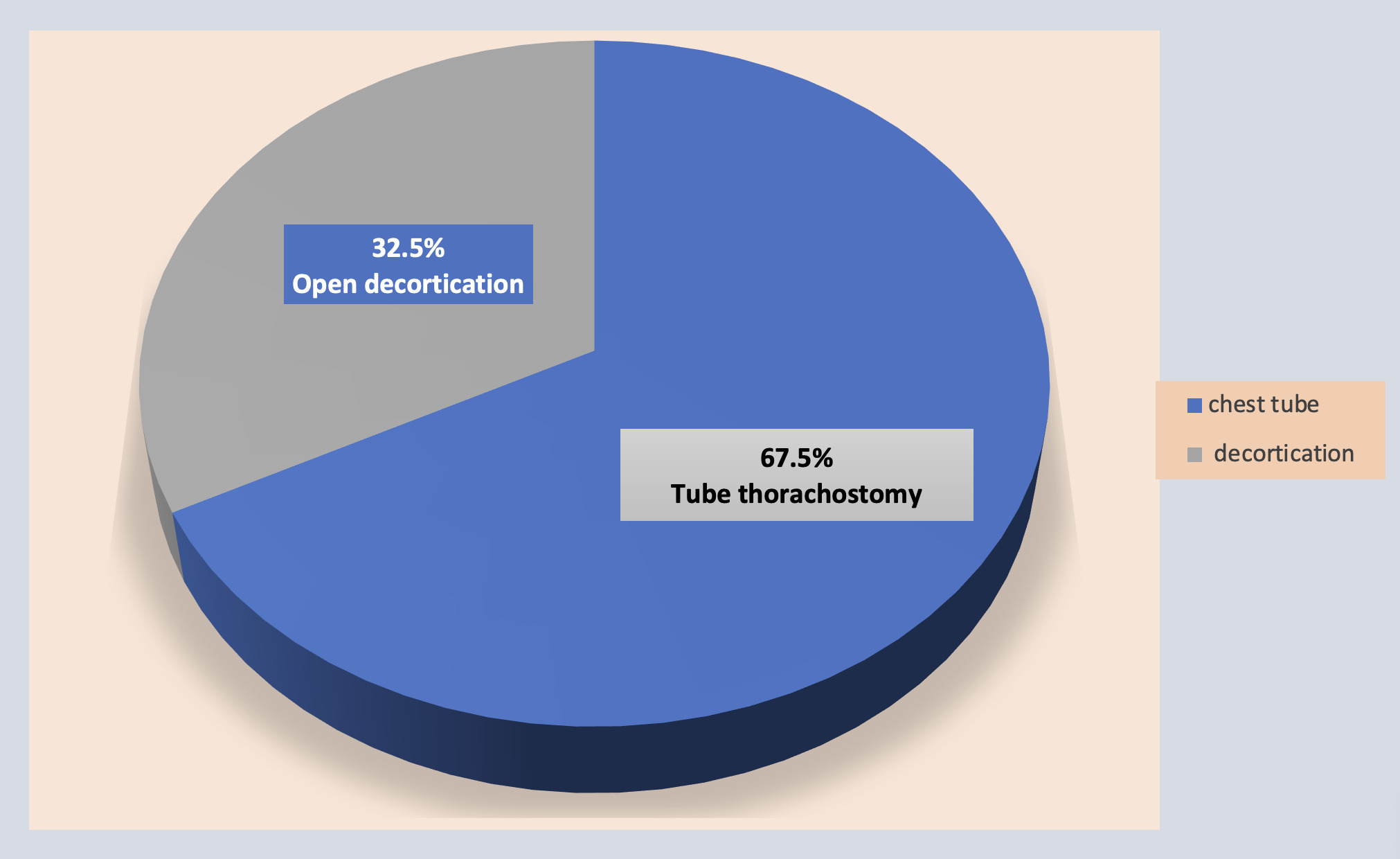
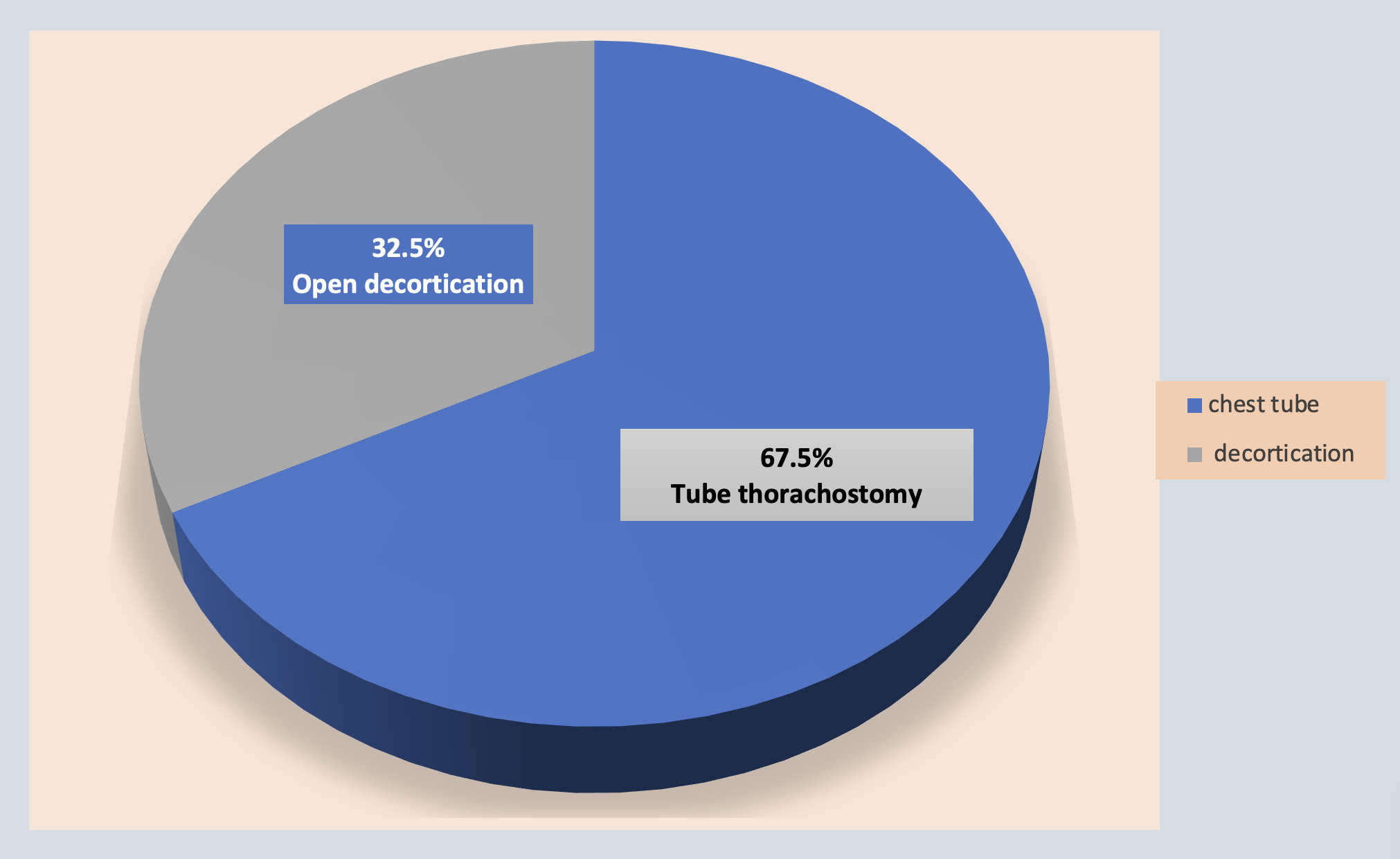
Tuberculosis was the predominant etiology, followed by pyogenic empyema. While the majority of patients (67.5%) were initially managed with tube thoracostomy, success rates varied significantly by etiology: 88.9% for pyogenic empyema, 79.41% for tuberculous empyema, and 38.46% for post traumatic empyema (Figure 2). Among the 27 patients (32.5%) who ultimately required open decortication, procedure as their primary intervention in our institution, tuberculosis was the leading indication (n = 16 [19.2%]), followed by post trauma (n = 8 [9.6%]) and pyogenic empyema (n = 3 [3.6%]).
Postoperative Complications and pattern of thoracic empyema patients at HUCSH
To ensure an accurate representation of clinical outcomes and avoid data duplication, we meticulously categorized patient trajectories. Among those with poor outcomes, 7 patients underwent reintervention followed by in-hospital mortality, while 5 patients expired from empyema without reintervention. An additional 11 patients required reintervention but survived to discharge. A similar categorization was applied to postoperative complication patterns.
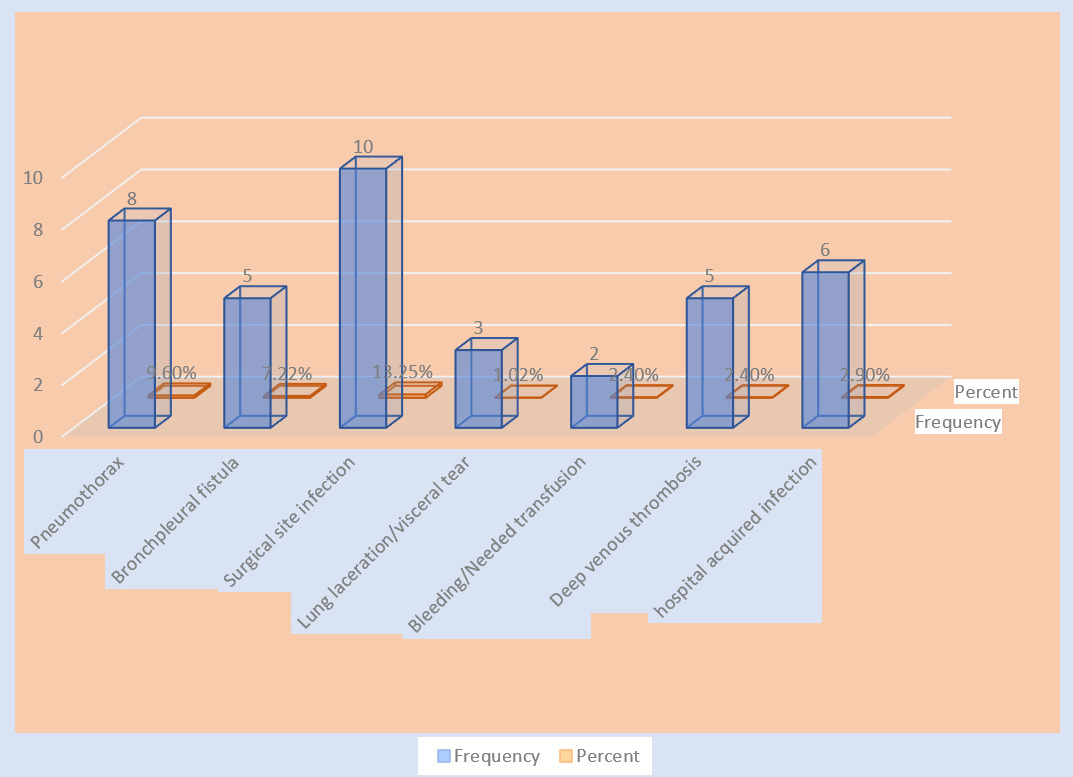
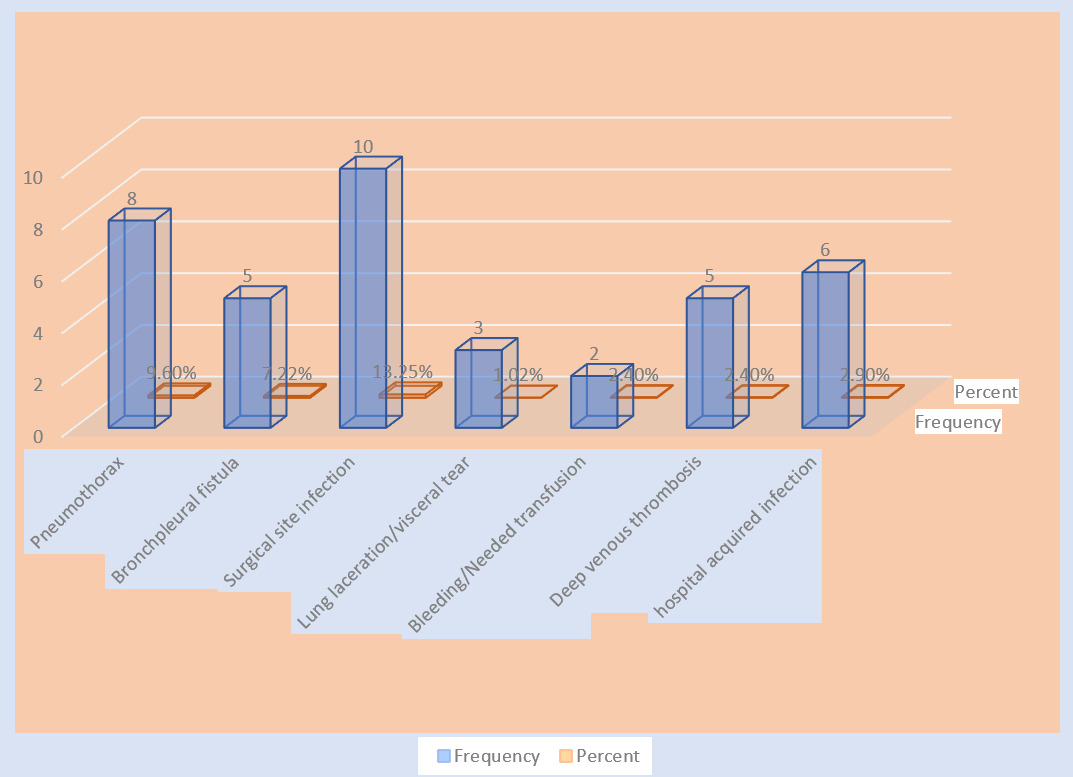
The most frequent postoperative complication was surgical site infection (n = 10 [13.2%]), followed by pneumothorax (n = 8 [9.6%]) and bronchopleural fistula (n = 5 [7.2%]). Intraoperative complications included lung lacerations (n = 3 [1.02%]) and blood transfusion requirements (n = 2 [2.4%]). Hospital-acquired infection occurred in 6 cases (n = 6 [2.9%]). The median length of hospital stay was 24 days (IQR, 20–32) (Figure 3).
Overall, 27.7% (n = 23) of the cohort experienced unfavorable surgical outcomes. This included a 21.7% (n = 18) reintervention rate and a 14.4% (n = 12) in-hospital mortality rate. Additionally, 24.1% (n = 20) of patients experienced incomplete resolution of empyema following their initial treatment.
Bivariate and multivariate binary logistic regression analysis on determinants of thoracic empyema surgical management outcomes at HUCSH
Age, comorbidity, duration of symptoms, etiology of empyema, stage of empyema, loculation of empyema, and initial surgical procedure were evaluated as potential factors affecting overall surgical outcomes. Although the stage of empyema showed strong negative predictive effects, it did not reach statistical significance on multivariate analysis. In contrast, age (AOR = 5.891; 95% CI, 1.587–21.873; P = 0.008), comorbidity (AOR = 3.597; 95% CI, 1.042–12.416; P = 0.043), and etiology of empyema (AOR = 5.026; 95% CI, 1.096–7.412; P = 0.034) were found to be independent predictors of unfavorable overall surgical outcome on multivariate binary logistic regression.
Similarly, age, comorbidity, duration of symptoms, etiology of empyema, stage of empyema, loculation of empyema, and initial surgical procedure were evaluated as potential factors affecting the need for reintervention. Stage of empyema (AOR = 6.354; 95% CI, 1.533–26.328; P = 0.011) and initial surgical procedure (AOR = 10.515; 95% CI, 2.695–41.018; P = 0.001) were independent predictors of reintervention need on multivariate binary logistic regression. Organizing stage of empyema and closed tube drainage on initial procedure were found to increase the odds of reintervention.
Age, comorbidity, duration of symptoms, etiology of empyema, stage of empyema, loculation of empyema, and initial surgical procedure were also evaluated as potential factors affecting resolution of empyema on initial treatment. Comorbidity (AOR = 4.129; 95% CI, 1.272–13.404; P = 0.018) was the only independent predictor of incomplete resolution of empyema on initial treatment in the multivariate binary logistic regression analysis. Presence of comorbidity increased odds of incomplete resolution of empyema (Table 2).
Discussion
This study evaluated pattern and determinant factors of surgical outcomes in thoracic empyema. Overall, 72.3% of patients achieved favorable surgical outcomes, while 32.5% required open decortication as primary and reintervention treatment, most commonly in cases of tuberculous empyema. Multivariable analysis showed that older age, underlying comorbidities, and tuberculous etiology were independent predictors of unfavorable surgical outcomes. Organized empyema, initial closed tube drainage, and comorbid conditions were associated with an increased likelihood of reintervention and incomplete resolution following initial treatment. The in-hospital mortality rate was 14.4% among empyema patients.
Thoracic empyema has been recognized since 3000–500 BC, when open thoracic drainage was the primary treatment and carried mortality rates of up to 70%, likely due to respiratory failure resulting from open pneumothorax.1–3 The introduction of closed chest tube drainage in 1876, which gained wider acceptance during the 1919 influenza epidemic, significantly improved management. Currently, approximately 80,000 cases are diagnosed annually in the UK and US combined, with 20% morbidity and mortality and nearly 20% of patients requiring surgical intervention.4–6 Despite advances in surgical techniques that have reduced morbidity and mortality, these benefits are not uniformly observed worldwide, because of variations in etiology and resource limitations, particularly in low- and middle-income countries.7–9
The demographic profile of empyema varies across regions. In Tikur Anbessa Specialized Hospital, Addis Ababa, the mean age of patients with chronic empyema was 59.6 ± 10.6 years, with a male-to-female ratio of 5.9:1. A study from Gondar University Teaching Hospital reported that nearly 60% of empyema patients were people living with HIV/AIDS.10 In Indian tertiary hospitals, an analysis of 437 patients reported a mean age of 38 years, with a male predominance of 5:1, tuberculosis accounting for 57% of cases, and diabetes mellitus as the most common comorbidity (22%).19 Another study from Tikur Anbessa, involving 127 patients, reported a peak age of 32 years, 59.1% tuberculosis-related empyema, and hospital mortality of 23.8%, of which 44.8% occurred in people living with HIV/AIDS.11,12 Comparative studies of tuberculous vs nontuberculous empyema in India also demonstrated younger age and longer drainage duration in tuberculous cases.13,14
Similarly, in our cohort, the median age was 45 years (IQR, 26–64), with a male-to-female ratio of 2.3:1. About 45.8% of patients had at least one comorbidity, and 13.3% were living with HIV/AIDS. Tuberculous empyema was the most common etiology (51.8%), highlighting the persistent burden of tuberculosis-related empyema in low- and middle-income settings.
Pyogenic empyema accounts for 40%–60% of cases, while posttraumatic empyema occurs in 1.6%–4.2%. Similarly, a 24-year multicenter study in the US involving 5474 trauma patients reported 87 cases (1.6%) of posttraumatic empyema, with 91% successfully treated without open thoracotomy.15 The most commonly identified pathogen was methicillin-resistant Staphylococcus aureus,16,17 while in our cohort, post traumatic empyema accounted for 15.7% of cases, and 61.5% of these required open decortications. Although microbiological cultures were not routinely performed in all patients, Staphylococcus aureus was the most frequently identified organism.
Microbiological patterns of thoracic empyema vary by region. A study of 110 patients at Bahawel Victoria Hospital, Punjab, Pakistan, reported gram-negative organisms as the most common pathogens, including Pseudomonas aeruginosa (18%), Klebsiella (10%), and E. coli (10%), many of which showed resistance to empirical antibiotics and were associated with poorer outcomes. A review of 105 patients in Calabar, Nigeria, similarly found that 43.8% of pathogens were gram-negative organisms, predominantly Klebsiella. Large reviews emphasize that antibiotic-resistant pathogens remain a major challenge in empyema management.18
The diagnosis of thoracic empyema requires integration of clinical assessment, laboratory findings, microbiological testing, and imaging modalities; however, diagnostic approaches may vary depending on resource availability and institutional practice patterns. In this study, chest ultrasound was performed in 78.3% of patients and CT scans in 69.8%, whereas microbiological confirmation was obtained in relatively few cases. Consequently, diagnosis often relied on clinical presentation and radiologic findings. A review of empyema management in sub-Saharan Africa reported that delayed diagnosis is frequently related to low clinical suspicion and limited access to diagnostic tools, while early antibiotic therapy and appropriate chest tube drainage improve outcomes.19,20
Management of thoracic empyema usually requires a multimodal approach, with treatment decisions guided by disease stage, etiology, patient condition, and available resources. A literature review from Hungary emphasized that no single universally accepted treatment modality exists, because of the complexity of the disease.21,22 Instead, management typically combines antibiotics or antituberculosis therapy with surgical intervention according to disease stage: chest tube drainage for stage I, VATS for stage II and open decortication for advanced organized empyema.24 A study from Tabriz, Northern Iran, reported that open thoracotomy achieved a cure rate of 96.2% with lower mortality and shorter hospital stays.25
Several studies have compared VATS and open thoracotomy for empyema management. A comprehensive review from the UK reported that VATS offers higher success rates (91% vs 44%), lower mortality, and fewer perioperative complications, although conversion to open surgery occurs in 10%–17.1% of cases.26 A retrospective cohort study of 420 patients at Duke University Medical Center, USA, also demonstrated that VATS is comparable or superior to open decortication, with a conversion rate of 11.4%, supporting its use as a first-line treatment. In contrast, studies from Zurich University Hospital, Switzerland, reported conversion rates of up to 44%, particularly in patients with delayed referral or gram-negative infections.
Despite advances in surgical management, thoracic empyema continues to carry significant morbidity and mortality. Editorial reviews from Oxford and Johns Hopkins report overall mortality rates of nearly 20% and note that chest tube drainage alone has the highest risk of treatment failure and need for reintervention.27 A prospective cohort study of 179 patients with primary empyema reported cure rates of 90% with thoracentesis, 62% with tube thoracostomy, and 88% with open decortication, with mortality rates of 11% and 1.3%, respectively.28 Conversion to open surgery was significantly associated with tuberculous empyema and anaerobic infections. Studies from Vietnam showed that VATS is effective for nonorganized empyema and in patients with severe comorbidities.28,29
In our study, about 67.5% underwent tube thoracostomy, while 32.5% required open thoracotomy and decortication as the primary treatment or reintervention measure, combined with antibiotic or antituberculosis therapy. Success rates were 88.9% for pyogenic empyema, 79.41% for tuberculous empyema, and 38.46% for post traumatic empyema. Overall, 21.8% required reintervention, and 24% had incomplete resolution after initial treatment, consistent with previous reports indicating poorer outcomes in tuberculous, post traumatic, and organized empyema.
Postoperative complications of surgery for empyema vary widely across studies. A 3-year study of 62 patients with chronic empyema at Tikur Anbessa reported mortality of 3.2%, with common complications including lung laceration (24.2%), bronchopleural fistula (12.9%), recurrent empyema (16.1%), and persistent air leak (22.4%), with an average hospital stay of 12 days (3–63 days).29,30
In our study, complications included surgical site infection (13.2%), pneumothorax (9.6%), bronchopleural fistula (7.2%), intraoperative lung laceration, bleeding requiring transfusion, and prolonged hospitalization. The in-hospital mortality rate was 14.4%, 78.6% of which occurred in patients with comorbid conditions. Studies from Gondar reported 56% tuberculous empyema with a mortality rate of 12%, suggesting a higher burden of severe disease in resource-limited settings, likely related to delayed presentation and limited early surgical access.
Surgical outcomes of thoracic empyema are influenced by multiple prognostic factors. A retrospective multicenter study from the US and UK found that delays in drainage beyond 3 days significantly increased morbidity and mortality. A nationwide Spanish analysis of 19,864 patients identified advanced age (>66 years) and comorbidities as independent predictors of hospital mortality.18 Similarly, a Taiwanese national study involving patients demonstrated that diabetes increased the risk of pleural empyema (HR, 1.71). A study from Mulago National Referral Hospital, Uganda, reported a mortality rate of 10.5% and a reintervention rate of 23.5%, with advanced age and none pyogenic empyema predicting mortality and delayed presentation predicting reintervention.14 Studies from Lusaka, Zambia, also reported high rates of people living with HIV/AIDS (66.6%) and tuberculosis coinfection (48.7%), contributing to prolonged hospitalization and mortality.24,30
Similarly, our analysis identified advanced age, comorbidities, and tuberculous etiology as independent predictors of unfavorable surgical outcomes, while organized empyema and initial tube drainage predicted reintervention, and comorbidities predicted incomplete resolution. Early diagnosis and timely referral, supported by a high index of clinical suspicion of stage, may reduce delayed presentation, disease progression requiring invasive surgery, and the significant morbidity and mortality associated with thoracic empyema.
Study Limitation
This study is subject to some limitations. Data were retrospectively collected from manually recorded patient charts, which introduced challenges related to legibility and completeness since electronic medical records are not yet available at HUCSH. Many patient charts were missing or lost, which decreased the sample size, even while reducing the potential for selection bias. The retrospective nature of the study further limits control over potential confounders and precludes assessment of causal relationships since only the variables recorded in the chart could be extracted. The independent predicting factors were observed with a wide confidence interval. This may indicate an imprecision of effect estimates, which may be attributable to a small sample size.
Conclusions
Etiology, disease stage, and patient condition had a significant impact on thoracic empyema management outcomes in the study. Older age, underlying comorbidities, and tuberculous etiology were associated with poor surgical outcomes. The need for reintervention was increased for organized empyema and initial treatment with closed tube drainage. Additionally, comorbidity significantly increased incomplete resolution of empyema. These findings may highlight a crucial insight into patient stratification that could help management decisions improve outcomes in similar settings.
Recommendations
We recommend strengthening early and accurate diagnosis of empyema and prioritizing older patients, those with multiple comorbidities, and those with tuberculous etiology. We also recommend improving medical records through modern electronic data systems and conducting future large-population and multicenter prospective studies to identify independent determinant factors.
Ethical Approval
The study was conducted after institutional review board approval was obtained from the Research Ethics Committee at Hawassa University College of Medicine and Health Sciences, which waived individual consent (registration number IRB/589/25). The data were extracted anonymously, and confidentiality was assured at each step of data collection and processing. The study complies with the principles of the Declaration of Helsinki.
Informed Consent
Not applicable.
Data Availability
The data supporting the findings of this study are available upon reasonable request from the authors but are not publicly available due to confidentiality restrictions.
Conflict of Interest
None.
Funding
None.