Introduction
Intussusception is one of the most common causes of intestinal obstruction in infants, occurring predominantly in children under 1 year of age and more frequently in males. Studies from Ethiopia, sub-Saharan Africa, and South Africa consistently report a median or mean age between 6 and 13 months, with males comprising nearly two-thirds of cases. Delayed presentation remains a recurring challenge in many African settings, with symptom duration commonly extending beyond three days.1–5
The disease condition results from one bowel segment telescoping into another, leading to venous congestion, bowel ischemia, and eventual necrosis if untreated. Children commonly present with vomiting, intermittent abdominal pain or inconsolable crying, abdominal distension, and currant jelly stools, although the full classical triad is often absent.6–13 Ultrasonography is the primary diagnostic tool; however, atypical forms such as compound or retrograde intussusception may be difficult to detect and are sometimes diagnosed only during surgery.14–19
Management includes nonoperative reduction and surgical intervention, with wide variation in practice and outcomes across regions.20,21 Nonoperative reduction success depends on technique, use of sedation, operator experience, and timing of presentation, with reported success rates ranging from 50% to 90%. Surgical management is frequently required in delayed or complicated cases and often entails postoperative complications from bowel resection. While hydrostatic reduction is associated with a relatively high rate of recurrence, it remains an important option in pediatric intussusception management.22–30
Although numerous local, regional and global studies describe the epidemiology and management of pediatric intussusception, outcomes vary widely, particularly in resource-limited environments. Particularly evidence from Ethiopia and similar sub-Saharan regions on predictors of management outcomes and mortality remains limited.
This study was therefore conducted to assess the clinical profile and predictors of treatment outcomes in pediatric intussusception by comparing hydrostatic and surgical management in our setting. The findings may help guide the development of local management protocols and guidelines for intussusception management and provide a foundation for future large multicenter prospective studies in our setting.
Methodology
This study was conducted at Hawassa University Comprehensive Specialized Hospital, located at 7°3’N and 38°28’E on the eastern shore of Lake Hawassa, Sidama. HUCSH is a major teaching and referral center serving an estimated 20 million people from the Sidama region, SNNPR, Southern Oromia, the Somali region, and parts of Somalia and Kenya. Established in 2003, the hospital has approximately 450 beds and delivers clinical and emergency services to more than 102,000 patients annually. A dedicated pediatric surgery unit was established with one Pediatric surgeon in 2017 and which has currently three pediatric surgeons, enhanced pediatric surgical care, postgraduate training, and pediatric surgery research capacity.
A retrospective cohort study was conducted from January 1, 2019, to December 31, 2025, to evaluate the relationship between preoperative risk factors and treatment outcomes in patients diagnosed with pediatric intussusception. A cohort design was selected to establish temporal associations between exposures and outcomes using existing medical records, which would not be adequately addressed through a cross-sectional approach. Accordingly, all pediatric surgical patients whom diagnosed with intussusception during the study period were source population. All patients with complete records for all major study variables and aged between 0 to 14 years were included in the study, while those with charts with incomplete essential data were excluded.
A census approach was applied to maximize number of cases capture so that all eligible pediatric intussusception cases were reviewed. During the study period, 142 pediatric patients underwent intussusception management, and 122 were included based on data completeness and eligibility. Data were collected after obtaining institutional review board approval by trained nurses, medical interns, and junior surgical residents using a structured checklist. Medical record numbers were identified from daily departmental reports, pediatric emergency and pediatric surgery ward logs, and operating theater registries. Extracted data were entered into the Kobo Toolbox system.
To ensure data quality, the checklist was pretested in the same setting, each record was assigned a unique code, and the final dataset was exported to SPSS version 26.3 for analysis. Descriptive statistics were generated, followed by bivariate and multivariate binary logistic regression to identify predictors of treatment outcomes. Study variables included demographic characteristics (age, sex, and birth order), preoperative clinical characteristics, whether hydrostatic reduction was performed, intraoperative findings and decisions, postoperative complications (surgical site infection, wound dehiscence, and anastomotic leak), and duration of hospital stay. The primary outcomes were defined as favorable and unfavorable management outcomes of intussusception, comparing hydrostatic vs surgical, while secondary outcomes included postoperative complication patterns, duration of hospitalization, and in-hospital mortality. After confirming the interdependence of outcome variables via chi-square testing, a primary measure of overall surgical outcome was established alongside secondary endpoints such as in-hospital mortality.
An analytical framework was employed to identify predictors of hydrostatic reduction vs overall surgical management outcomes. Initially, chi-square and Fisher’s exact tests were used to assess associations between potential predictors and both primary and secondary outcomes. Confounding variables were identified and addressed through restriction and sensitivity analysis. Variables demonstrating significant or clinically relevant associations in bivariate binary logistic regression were subsequently entered into multivariate binary logistic regression models to identify independent predictors of treatment outcomes.
Operational definitions are as follows:
-
Hydrostatic reduction: Reduction of intussusception using saline enema pressure while following the reduction progress of the intususceptum by abdominal ultrasound.
-
Delayed reduction enema (DRE): Repeated hydrostatic reduction after a minimum of 4 hours of failed initial hydrostatic reduction attempt.
-
Delayed presentation: Pediatric patients presenting to the hospital >2 days after symptom onset (vomiting, abdominal pain, and rectal bleeding or currant jelly stool).
-
Compound intussusception: Bowel segment telescoping into an adjacent proximal or distal bowel lumen after an initial intussusception, or the simultaneous presence of separate intussusceptions at different anatomical sites.
-
Early postoperative recurrence: diagnosis of intussusception within 15 days of initial operation for intussusception management.
-
Unfavorable surgical outcome: Major adverse event after surgery, including major surgical complications, prolonged hospital stays, reoperation, and in hospital mortality.
Results
Overview
In this cohort study evaluating treatment outcomes of hydrostatic reduction vs surgical management, postoperative complication patterns, and mortality rates, variable classifications such as age group, duration of symptoms, triad of presentation, distal anatomic site of the intussusception, and length of hospital stay were based on previously published literature and pediatrics textbooks.
Sociodemographic characteristics of pediatric intussusception managed at HUCSH
Male cases predominated, accounting for 79 (64.8%) of the total number. The majority of patients (77 [63.1%]), presented between the ages of 6 and 17 months, at a median age of 9 months (IQR, 5–17). Oromia regional state accounted for 53.3% of the population, while 68 (55.7%) lived in rural areas. Approximately 90.2% of these patients were referred, with 72.7% of those referrals being for pediatric surgeon evaluations; and 8.12% of patients were diagnosed with severe community-acquired pneumonia.
Clinical characteristic patterns of pediatric intussusception managed at HUCSH
The median duration of symptoms prior to presentation was 4 days (IQR, 2–5), with approximately 32% of patients presenting between 2 and 3 days of symptom onset. The most common presenting symptoms were vomiting (21.4%), passage of blood per rectum (19.1%), anorexia or loss of appetite (18%), and abdominal pain (18%). Upon physical examination, the most frequent clinical signs were a palpable abdominal mass (42.5%) and a palpable per-rectal mass (37.7%), followed by generalized abdominal tenderness (15%) and prolapsed intussusception (3.1%). In addition, 4.1% of patients presented with shock (4 cases of hypovolemic shock and 1 case of septic shock), 4.9% with severe dehydration, and 5.7% with severe malnutrition (Table 1).
Laboratory investigations revealed leukocytosis in 72.1% of patients, while agranulocytosis was observed in 24.6%. Abdominal ultrasonography was performed in 97 (79.5%) patients by radiologists or radiology residents. The most commonly identified ultrasonographic findings were the target (donut) sign (34.4%), mesenteric lymphadenopathy (15.9%), free peritoneal fluid (29%), decreased bowel vascularity (5.1%), and absent bowel vascularity (1.1%). Radiologic evidence of bowel perforation (pneumoperitoneum) was identified in 1 case (0.4%).
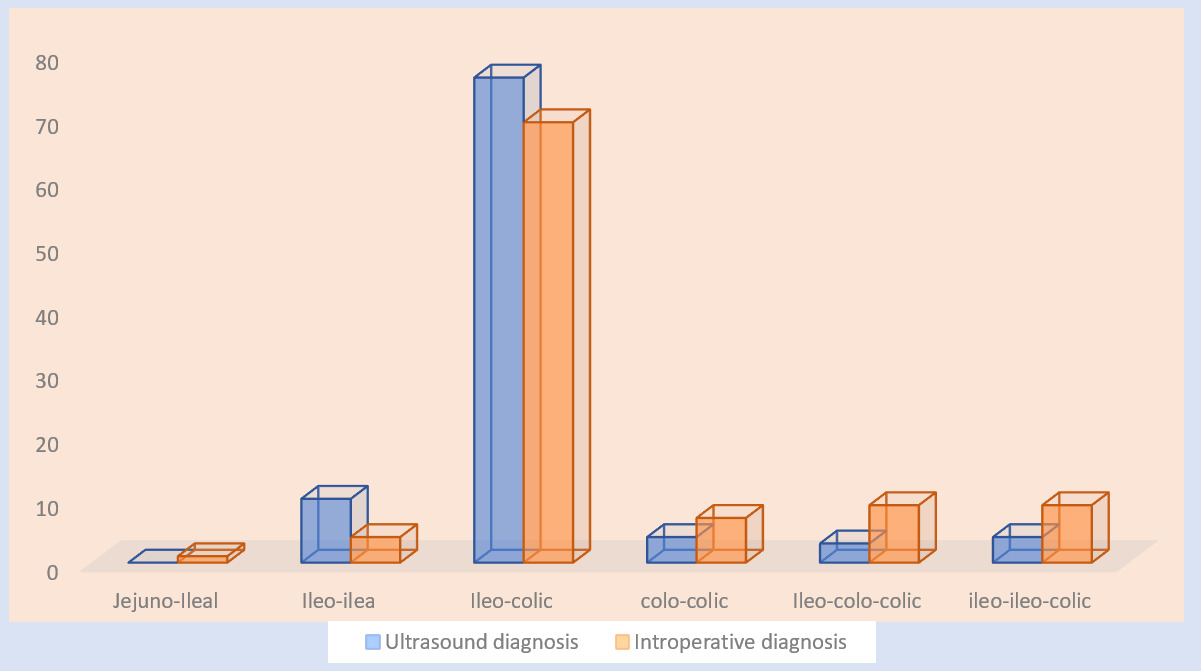
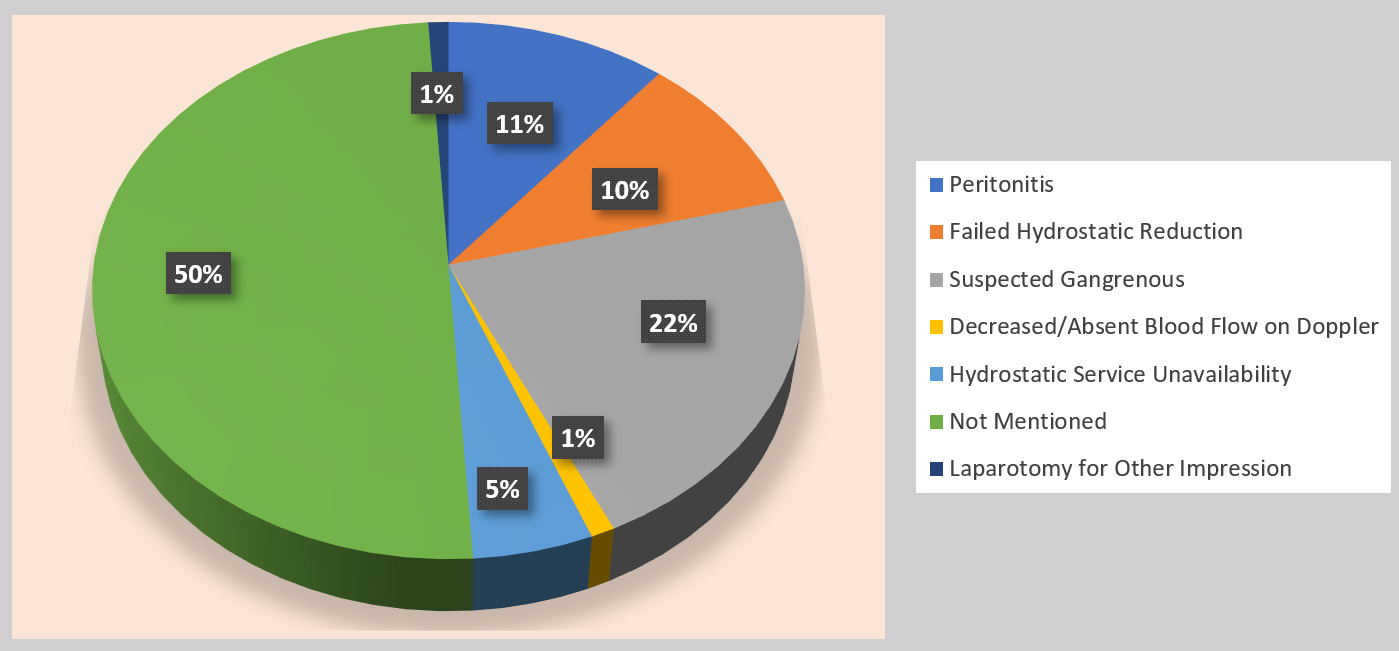
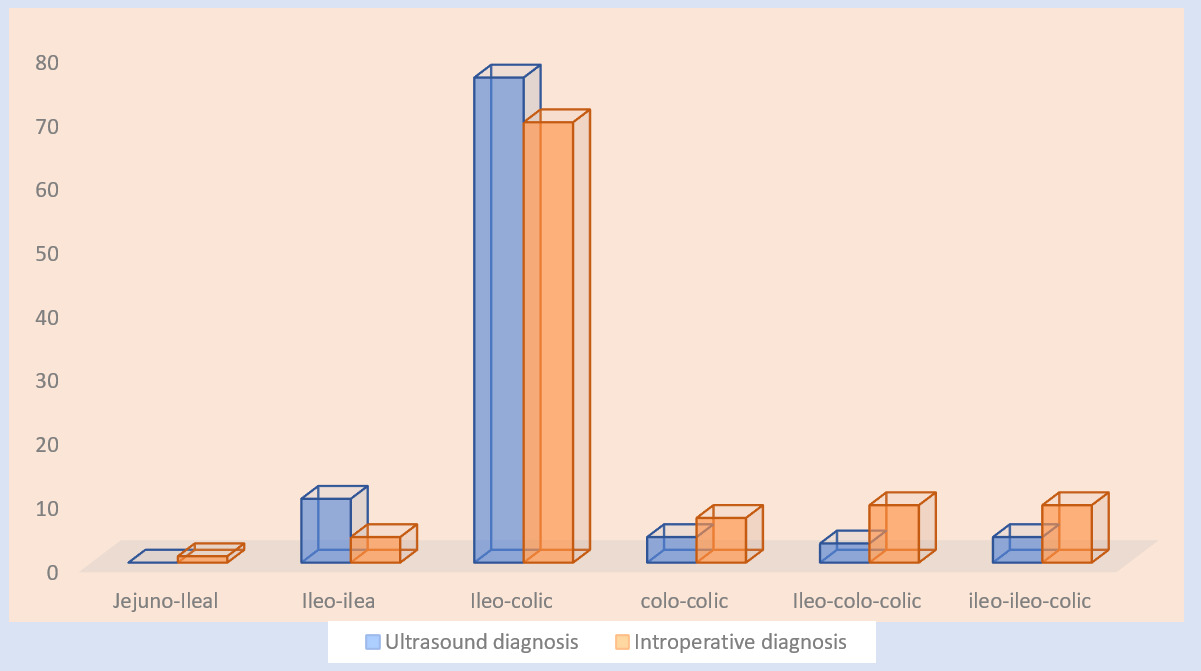
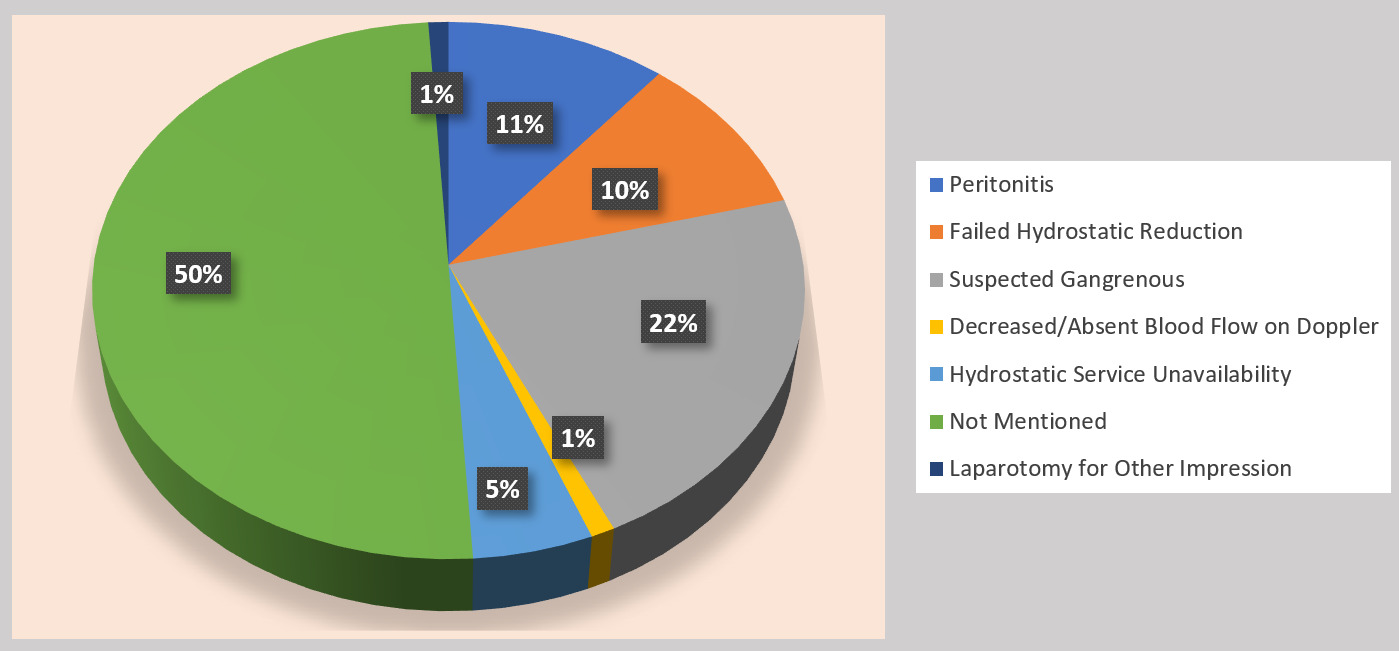
The most frequent type of intussusception diagnosis was ileocolic (79%), followed by ileoileal intussusception (10%). In 40.8% of patients, the distal end of the intususceptum extended beyond the splenic flexure. The diagnosis of intussusception was established based on clinical evaluation and abdominal ultrasonography. Following the initial clinical assessment, 25.8% of patients were subjected to hydrostatic reduction, while 7 (7.2%) were managed with watchful waiting. All of the later cases involved ileoileal intussusception (Figure 1). Surgical intervention was performed in 81.9% of patients, including those having undergone unsuccessful hydrostatic reduction. Patients with suspected gangrenous bowel (22%) and peritonitis (11%) underwent primary surgical management from the outset (Figure 2). Notably, among patients who underwent surgery, approximately 50% had no clearly documented indication of direct surgical intervention.
Hydrostatic enema reduction of pediatric intussusception managed at HUCSH
Despite international advocacy for a shift toward nonoperative management of intussusception, hydrostatic reduction was performed in only 20.7% of patients in our cohort. Warm normal saline was slowly instilled per rectum using a large-caliber Foley catheter, and hydrostatic pressure was generated by elevating the saline reservoir to approximately 150 cm above the patient on an IV stand. All procedures were performed with real-time ultrasonographic guidance by a radiologist or radiology resident or, in a few cases, by a surgeon. Procedural sedation with diazepam was documented in 3 cases (12%), and prereduction antibiotics were administered to 3 patients (12%).
Hydrostatic reduction was successful on the first attempt in 14 patients with a success rate of 56%, while 11 patients (44%) experienced failure. Delayed enema reduction (DER) was attempted in 3 patients (30%) and was successful in 1 patient, with a success rate of 33.3%. Recurrence following successful hydrostatic reduction occurred in 1 patient (6.7%) within 24 to 48 hours and was managed successfully with repeat hydrostatic reduction. In 1 (0.4%) patient, bowel perforation occurred during the hydrostatic reduction surgical procedure. The overall maximum number of documented attempts was two for all hydrostatic reduction cases.
The median length of hospital stay was 3 days (IQR, 2–4), with 68% of patients discharged on the third day.
Intraoperative course of surgically managed pediatric intussusception at HUCSH
All patients received prophylactic antibiotics and underwent surgery under general anesthesia with endotracheal intubation. Anesthetic care was provided by a master’s-level anesthetist in 56% of cases, a bachelor’s-level anesthetist in 41%, and an anesthesiologist in 3%. The majority of procedures (96%) were primarily performed by senior general surgery residents under the supervision of a pediatric surgeon. Even though there are no well-developed local guidelines for intussusception surgical management, this study used the international standards for surgical indications, such as perforation and peritonitis, as absolute indicators. In our setups, we found more than half of patients had no clear indications that had been documented. This may be attributed to different facility-related factors, such as poor documentation, unavailability of necessary materials, radiology experts, and surgical residents/hands on training urge to operate without obtaining adequate data for absolute or relative indication.
Nearly all operated patients were managed via an open right upper quadrant transverse incision. Intraoperative findings included fecal peritoneal contamination in 3% of cases, hemorrhagic peritoneal fluid in 6%, frank bowel gangrene in 17%, and perforated gangrenous bowel in 5%. The most common intraoperative diagnosis was ileocolic intussusception (69%). Additionally, 18% of patients were incidentally found to have compound intussusception, all of which were retrograde in nature (Ileo–Ileo–Colic and Ileo–Colo–Colic).
Intraoperatively, all ischemic bowel segments were packed with warm saline for approximately 10 minutes; however, persistent ischemia was observed in 13.7% of cases. Manual reduction was successful in 69% of patients, while 29% required bowel resection with anastomosis or stoma creation. One negative laparotomy was reported. Frank gangrenous bowel accounted for 17 (58.6%) as an indication for bowel resection (Table 2).
Among patients who underwent bowel resection, 2-layered anastomosis was performed in 21 patients (80.8%), and end-to-end anastomosis was performed in 24 patients (92.3%). Ileo-transverse anastomosis was the most commonly performed reconstruction (65.4%). Stoma creation was required in 4 patients (4%), indications included extensive bowel ischemia incompatible with primary resection in 3 cases and intraoperative hemodynamic instability in 1 case (Table 2).
Postoperative course of surgically managed pediatric intussusception at HUCSH
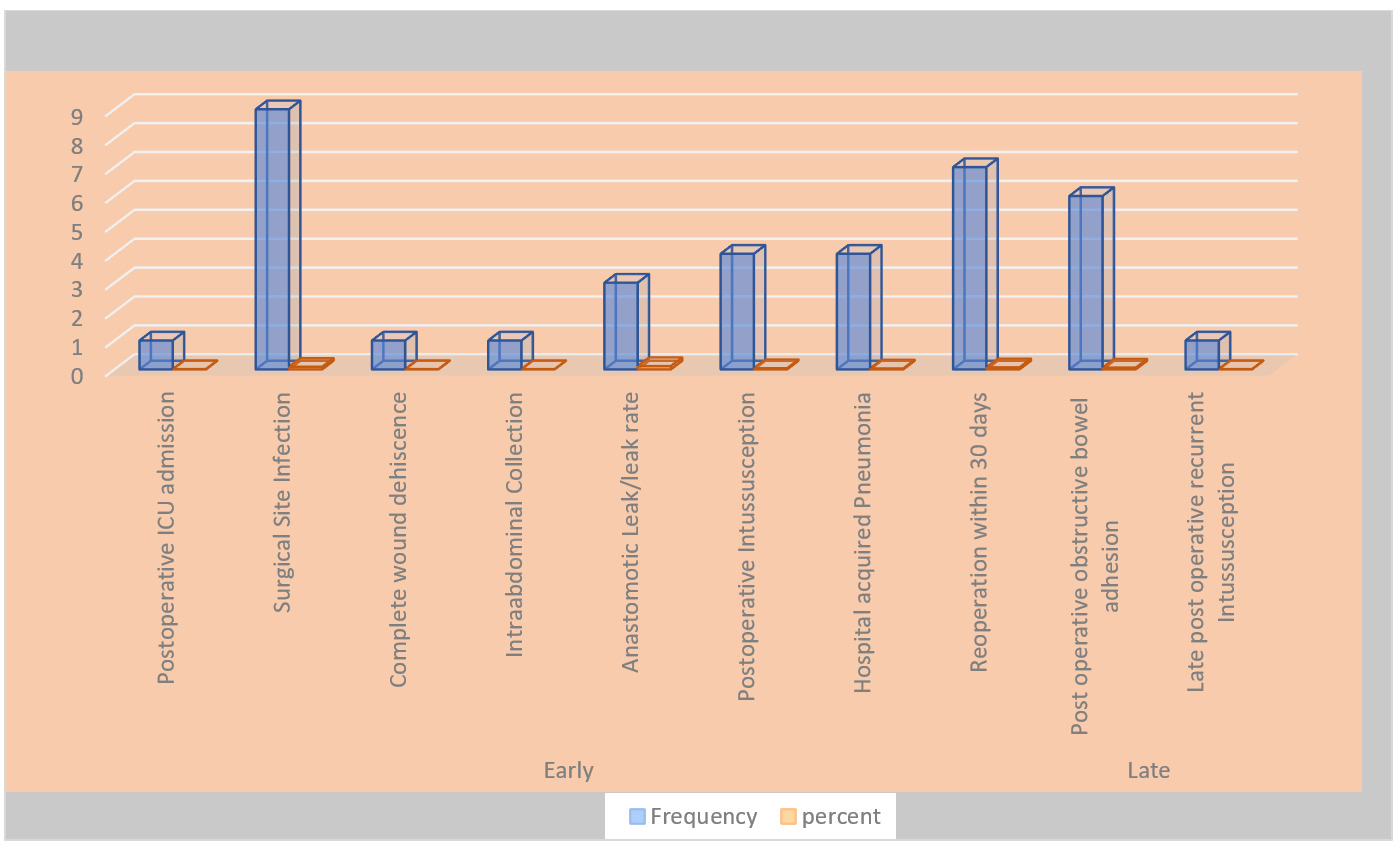
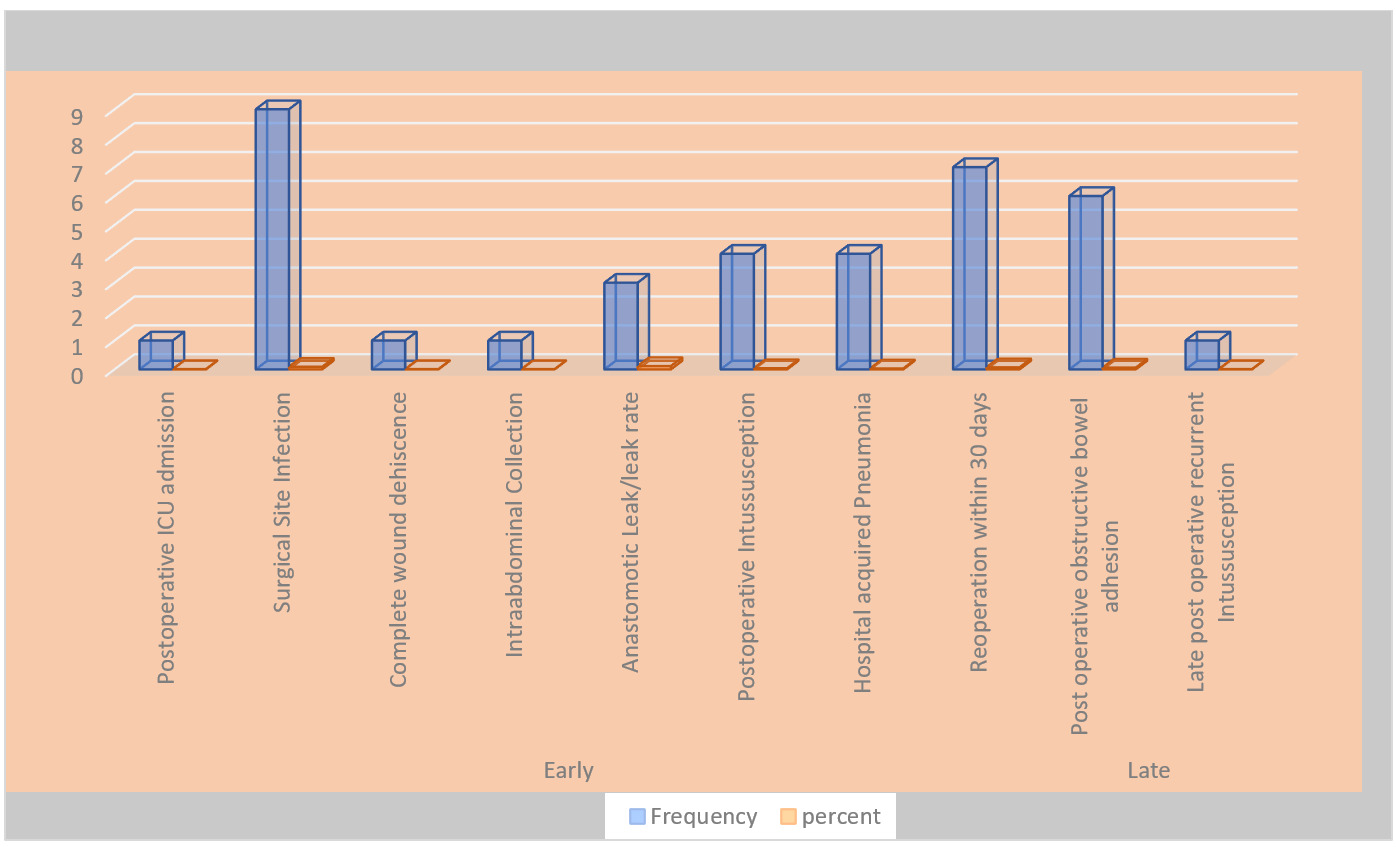
The overall postoperative morbidity was 18%, calculated per patient to avoid double counting among those who experienced more than one complication. The most common postoperative complications were surgical site infection (9%), anastomotic leak in 3 patients (11.5% of those who underwent anastomosis), and the need for reoperation in 7 patients (7%). Indications for reoperation included postoperative intussusception and anastomotic leak, often in association with other complications.
The in-hospital mortality rate was 4.9% (n = 6). All deaths occurred among surgically managed patients, and multiorgan failure secondary to irreversible septic shock was the most commonly documented immediate cause of death. The median length of hospital stay was 4 days (IQR, 3–7).
Late postoperative complications were observed in 7 patients (7%), of whom 6 (85.7%) required surgical intervention. Indications for late reoperation included postoperative adhesive intestinal obstruction in 5 patients and late recurrent intussusception in 1 patient (Figure 3).
Bivariate and multivariate binary logistic regression analysis on predictors of treatment outcomes of pediatric intussusception managed at HUCSH
To identify factors influencing the success of hydrostatic reduction, surgical management outcomes, and in hospital mortality in pediatric intussusception management at HUCSH, an analytical framework was employed. Initially, chi-square and Fisher’s exact tests were used to assess associations between potential predictor variables and each outcome of interest. Based on these preliminary analyses, relevant variables were identified and an appropriate statistical plan was developed. Potential confounding variables were recognized and addressed through restriction and sensitivity analyses. Variables with significant or clinically relevant associations in bivariate binary logistic regression were subsequently entered into multivariate binary logistic regression models to identify independent predictors for each outcome.
Accordingly, duration of symptoms, distal anatomical extension of the intussusceptum beyond the splenic flexure, ultrasound operator during reduction, presence of mesenteric lymphadenopathy, bowel vascularity status on ultrasonography, and use of procedural sedation were evaluated as potential factors influencing the success of hydrostatic enema reduction. However, none of these variables demonstrated a statistically significant association with successful hydrostatic reduction.
Duration of symptoms, shock (hypovolemic or septic) at presentation, peritonitis, hemorrhagic peritoneal fluid, peritoneal fecal contamination, and need for bowel resection were evaluated as potential factors influencing overall surgical outcomes. Although duration of symptoms and shock at presentation demonstrated strong negative predictive effects, they did not reach statistical significance on multivariate analysis. In contrast, need for bowel resection (P = .010; AOR = 6.036; 95% CI, 1.003–10.447) was an independent predictor of unfavorable surgical outcomes on multivariate binary logistic regression.
Additionally, duration of symptoms, shock at presentation, peritonitis, hemorrhagic peritoneal fluid, fecal contamination, intraoperative bowel vascularity, peritoneal status, and presence of postoperative complications were evaluated as potential factors influencing mortality. Shock (hypovolemic or septic) at presentation (P = .013; AOR = 4.913; 95% CI, 2.258–94.7) and peritoneal fecal contamination (P = .046; AOR = 41.84; 95% CI, 1.064–1655.3) were independent predictors of in-hospital mortality among patients with intussusception (Table 3).
Discussion
This study assessed predictors of treatment outcomes of pediatric intussusception. Hydrostatic reduction was attempted in 20.5% of patients, with a first attempt success rate of 60%, while 81.9% underwent surgical management, of whom 29% required bowel resection with anastomosis or stoma creation. There was no identified independent predictor for the success of hydrostatic reduction; however, the need for bowel resection was the only an independent predictor for overall unfavorable surgical management outcomes, while shock at presentation and intraoperative peritoneal fecal contamination were an independent predictors of in-hospital intussusception mortality.
A meta-analysis of 672 pediatric intussusception cases in Ethiopia reported a mean age at presentation of 12 months, a male predominance of 66%, and a mean symptom duration of 3.1 days. Similarly, a systematic review of 2078 children from 11 sub-Saharan African countries published between 1991 and 2024 found a mean age of 13.2 months and 64% male cases. A separate meta-analysis of 476 cases from South Africa showed a younger distribution, with a median age of 6.5 months (IQR, 2.6–32.6 months).1–4 In our study, the median age was 9 months (IQR, 5–17) with male predominance (64.8%).
A meta-analysis of 476 South African patients reported a median symptom duration of 3 days (IQR, 1–4 days), comparable to our study population’s median of 4 days (IQR, 2–5 days). Across studies, the most common presenting symptoms were vomiting, currant jelly stools, and abdominal pain or inconsolable crying,5–9 while a mass per rectum was detected in 37.7% of our cohort.
An article review involving 4719 patients concluded there is a high likelihood of missed diagnosis in cases of retrograde and compound intussusception. In that review, 0.25% of patients had retrograde intussusception not detected on ultrasound but subsequently diagnosed during operative reduction.10–13 In comparison, our study found that 18% of patients had compound intussusception.
Across multiple studies, nonoperative reduction demonstrates variable success depending on technique and sedation. A South African meta-analysis of 476 cases reported success rates of 66% for pneumatic reduction and 28% for enema, with a 4% bowel perforation rate for hydrostatic reduction. In Thailand, pneumatic reduction was 1.48 times more successful than hydrostatic barium enema (61% vs 44%). A systematic review of 17 studies including 2094 patients found an 87% success rate for nonoperative reduction with sedation, with pneumatic reduction reaching 94%. Saudi Arabian data reported an 80% success rate for pneumatic reduction, while another study showed hydrostatic success of 79% with sedation and 74% without; recurrence after successful hydrostatic reduction was 11.3%. A Luxembourg study demonstrated an 83% success rate on the first attempt, with sedation increasing success tenfold.9–13 International predictors of radiologic reduction are well-described. A Spanish study of 116 patients reported a 77% success rate, identifying free peritoneal fluid, absent Doppler flow, and distal intussusception location as factors for failure. A Tulane University study of 1025 cases demonstrated that shorter symptom duration increased the likelihood of success, while Slovenian data highlighted operator experience as a determinant.14–17 Another US study reported a 57% success rate for delayed reduction enema (DRE). The European Society of Pediatric Radiology found no significant difference between fluoroscopic and hydrostatic reduction and recommended universal sedation.18,19 In contrast, an Italian review found no association between success and either sedation or perforation. Chinese studies reported a 7.3% recurrence rate and decreasing success with repeated attempts, while an Indian study showed a DRE success rate of 27%.20 A Greek study reported a 97% pneumatic success rate.21,22 In our cohort, hydrostatic reduction was performed in 20.5% of patients, with a 56% success rate on the first attempt, 33% for DRE and around 60% overall success rate.
Several studies show wide variability in radiologic success influenced by symptom duration, anatomy, and institutional practice.23 Several studies highlight the burden of bowel resection. A Nigerian study reported a 43.8% resection rate, identifying age under 12 months and abdominal pain as predictors of resection and subsequent postoperative complications. A Tanzanian study found a 46.4% resection rate and a 14.3% mortality rate associated with delayed presentation and peritonitis.24,25 A multicenter study of 4016 children noted that longer symptom duration predicted resection, while lead points increased the likelihood of resection by a factor of 2.3.26 A Canadian study of 961 cases reported operative reduction in 29.4%, with delays over 1 day increasing resection risk. Conversely, Thai data showed a 3% recurrence rate after operative reduction and 0 after resection.27 In our cohort study intraoperative hemorrhagic fluid, delayed presentation, and compromised vascularity were strongly associated with resection, with a 5.7% recurrence after manual reduction and none after resection.
Ethiopian meta-analysis reported resection with anastomosis or stoma in 35% of patients, with a 26% complication rate, primarily surgical site infection (SSI), which occurred in 15% of patients. A sub-Saharan African review of 2078 children found resection required in 38.2%, a 24.5% complication rate, and 12.4% mortality. Conversely, South African data reported a higher resection rate of 61%.28 In our study, resection was performed in 29% of patients, with right hemicolectomy required in 65.3%. Postoperative morbidity was 18%, including anastomotic leak (11.5%) and SSI (9%). Our study showed slightly lower resection and complication rates compared to sub-Saharan countries, with right hemicolectomy as the most frequent procedure performed.
Although not performed in our setup, laparoscopic reduction shows equal efficacy compared to open surgery in the US, Japan, and international meta-analyses, with shorter hospital stays and earlier feeding.29,30 A US analysis of 8289 children reported that 42% underwent surgery and 15% required resection, with a 2.3% recurrence rate after manual reduction.30,31 A review of seven sub-Saharan countries via the CDC African Intussusception Network found a 48% resection rate and 13% mortality, identifying prolonged symptoms and resection as risk factors for death.32,33 In our study, intraoperative fecal contamination and shock were independent predictors of in-hospital pediatric intussusception mortality of 4.9%.
This study highlights predictors of intussusception treatment outcomes in a setting where delayed presentation is common. It shows that bowel resection is linked to unfavorable outcomes, while shock (hypovolemic or septic) and peritoneal fecal contamination were independent predictors of in-hospital intussusception mortality. The strong association between compromised bowel vascularity and the need for resection highlights the central role of bowel viability in determining prognosis.
Study Limitations
This study is subject to some limitations. Data were retrospectively collected from manually recorded patient charts, introducing challenges related to legibility and completeness. Poor handwriting and documentation practices affected the accuracy and reliability of data extraction. A number of patient charts were missing or lost, reducing sample size. Several important clinical variables including absolute indication for surgical intervention and bowel status during anastomosis were inconsistently recorded or entirely absent. Retrospective nature of the study limits full control over confounding variables and some independent predicting factors showed a wide confidence interval, which reflects the small sample size and reduced precision of conclusion.
Conclusions
Despite the recent shift in pediatric intussusception management toward hydrostatic reduction, about 81.9% of cases analyzed in this study were managed surgically. Hydrostatic reduction was associated with shorter hospital stay, lower morbidity, and no mortality. The need for bowel resection was the only independent predictor of unfavorable surgical management outcomes, while diagnosis of shock (hypovolemic or septic) at presentation and peritoneal fecal contamination were independent predictors of in-hospital intussusception mortality. This study provides an important insights on predictors of treatment outcomes, which may help to improve patient care and support the development of standardized local protocols for pediatric intussusception management in similar settings.
Recommendations
Improving pediatric intussusception outcomes requires timely diagnosis, proper management decisions, and attention to predicting factors of treatment outcomes. Establishing an electronic medical record system at HUCSH can enhance data quality. Prospective multicenter studies with larger sample sizes are recommended to better evaluate predictors of hydrostatic success, surgical outcomes, and in hospital intussusception mortality.
Ethical Approval
The study was conducted after the institutional review board approval letter was obtained from Hawassa University College of Medicine and Health Sciences institutional review board research ethical committee, with registration number IRB/019/25 which waived individual consent. The data were extracted anonymously, and confidentiality was assured at each step of data collection and processing. The study complies with the principles of Helsinki.
Informed Consent
Not applicable
Data Availability
The datasets generated during the study are not publicly available due to patient confidentiality but are available from the authors upon reasonable request and with appropriate ethical approval.
Conflict of Interest
None.
Funding
None.