Introduction
The incidence of crossing vessels in the etiology of Pelvic-Ureteric Junction Obstruction (PUJO) in children has been reported as ranging from 11%–15%.1 However, the concurrence of PUJO and duplicated systems is much less common, and more so when associated with a crossing vessel. Detection of such anomalies with imaging is key to the management approach, and intraoperative decision-making is based on the anatomic variants.2 We report a rare occurrence of PUJO associated with an incomplete duplex system in the upper urinary tract, with a lower pole crossing vessel causing extrinsic obstruction of both upper and lower moieties. This report also describes a laparoscopic-assisted technique useful in resource-limited settings, where intracorporeal suturing would increase operative time and require a higher level of skill and experience.
Case Description
A 6-year-old girl presented to our outpatient clinic with complaints of right-sided abdominal pain for over 2 years. Previously, she had been treated twice for urinary tract infections (UTIs). She had no history of hematuria, and her growth and developmental history did not reveal any relevant information related to the illness. She was stable on physical examination; her vital signs were normal. Her abdominal examination did not reveal any masses around the flanks, and a urine analysis was negative for UTI.
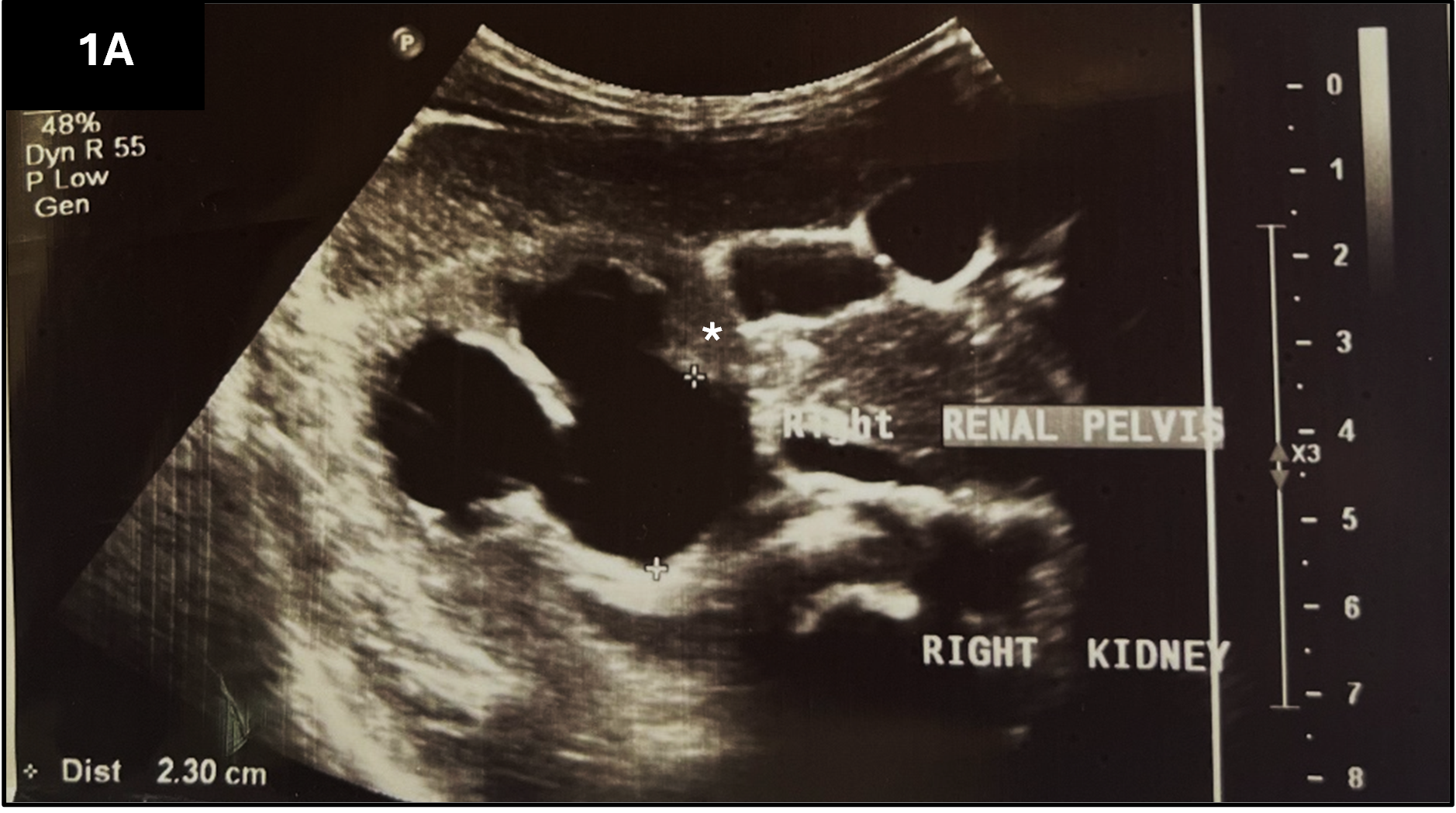
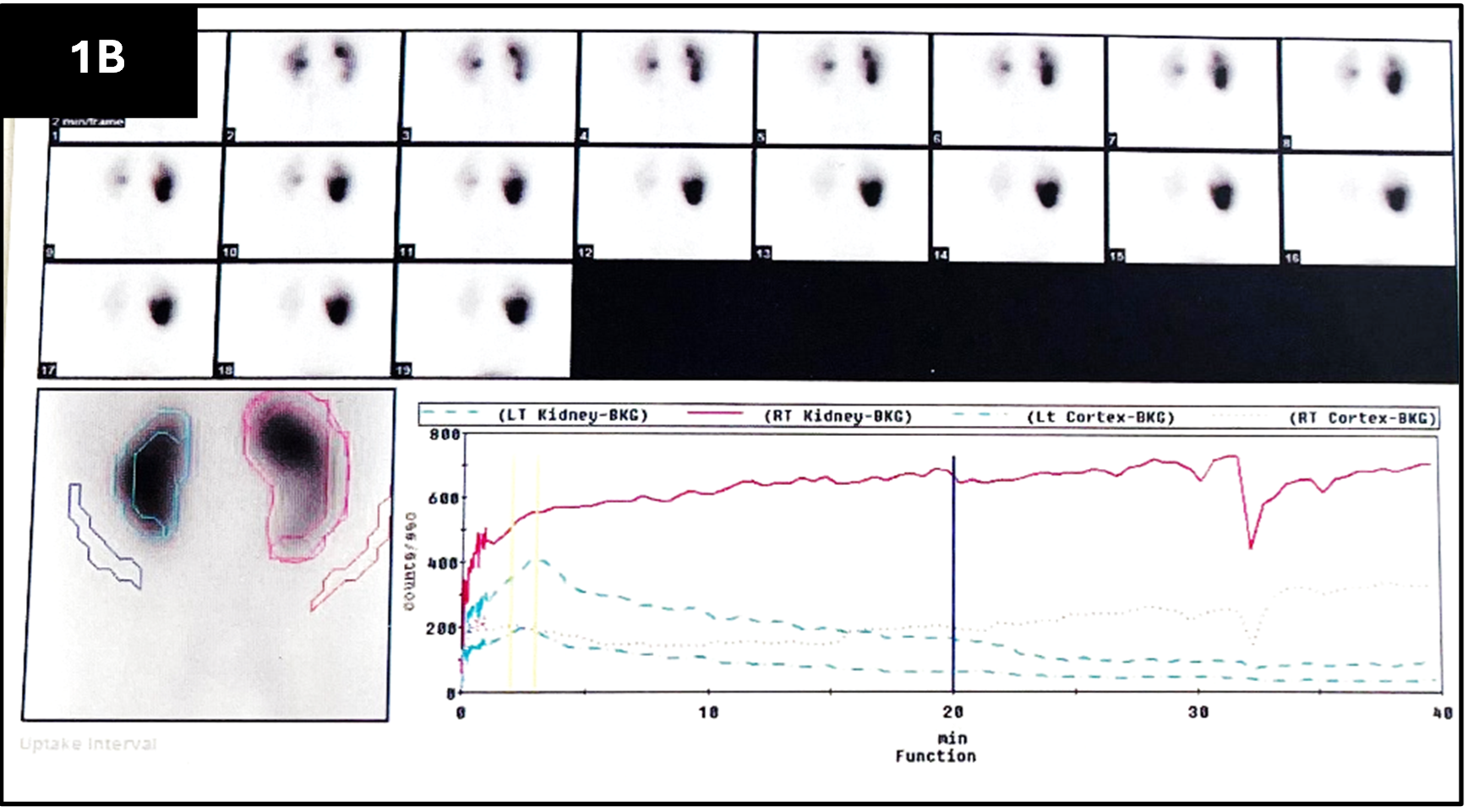
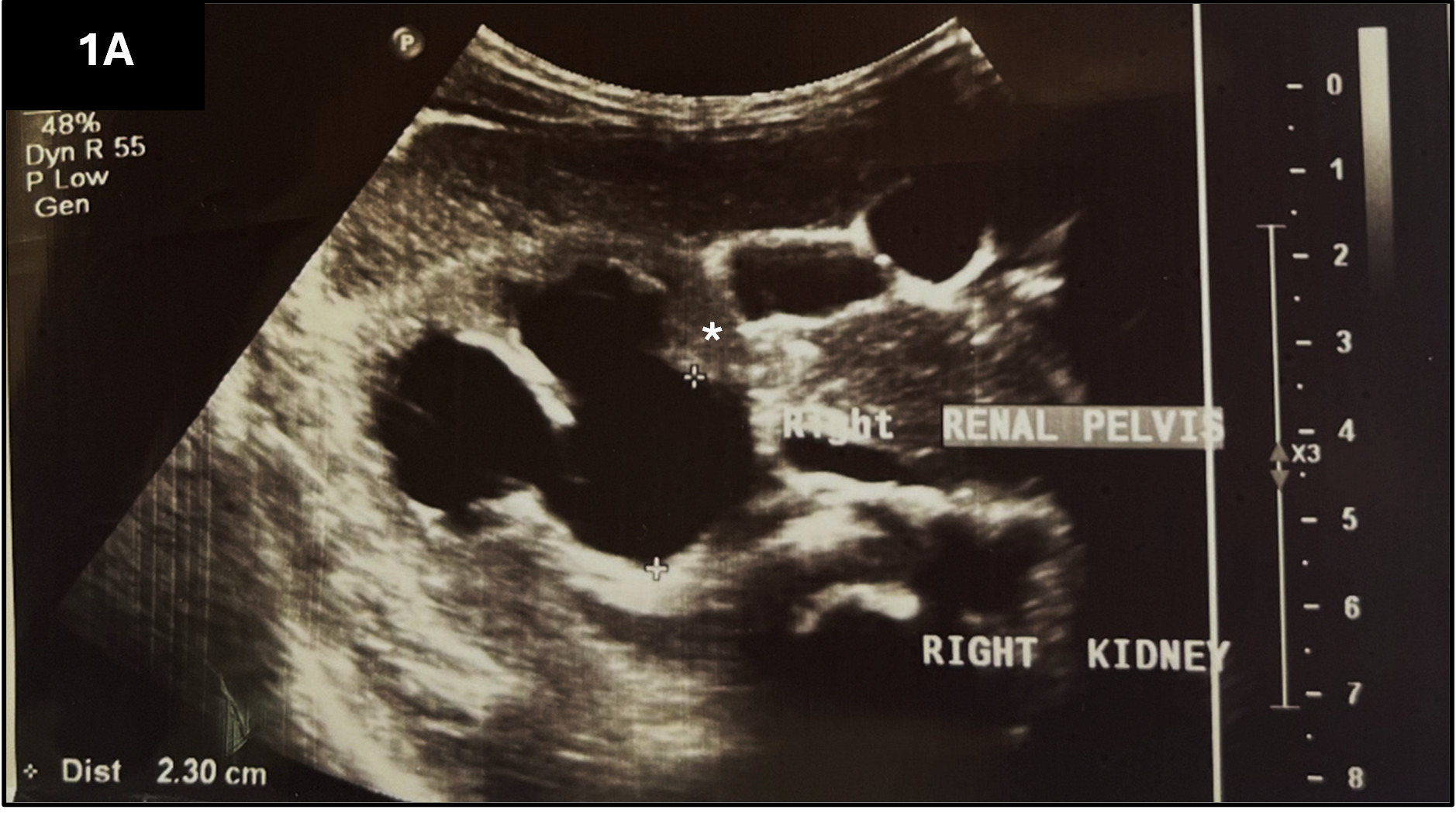
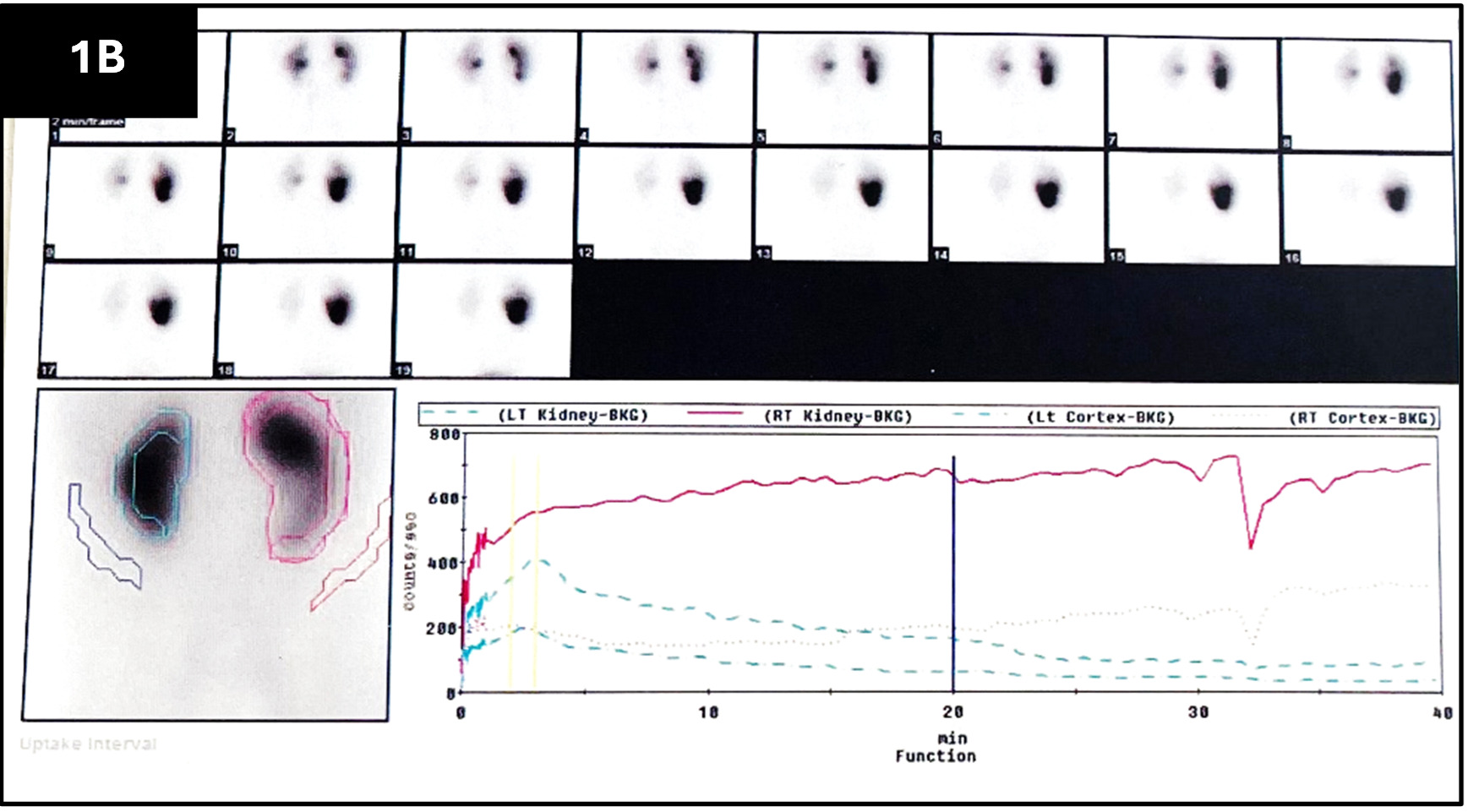
Based on these clinical findings, the differential diagnoses included PUJO, urolithiasis, and a proximal ureteric stricture, all of which can manifest with chronic flank pain. A series of imaging was done. An ultrasonography detected a grade 2 hydronephrosis (Figure 1A) with no hydroureter and with an intervening cortical bar suggestive of a duplex system. The left kidney and bladder anatomy were normal. Due to financial constraints, we prioritized [99mTc]-DTPA renal scintigraphy over CT intravenous urogram (CT IVU) to obtain quantitative functional data. A DTPA renogram demonstrated a hydronephrotic right kidney with preserved differential function of 58% (compared to left 42%) but severely impaired drainage. The excretory phase showed progressive tracer accumulation within the dilated collecting system with no response to a diuretic (furosemide), consistent with significant obstruction warranting intervention (Figure 1B).
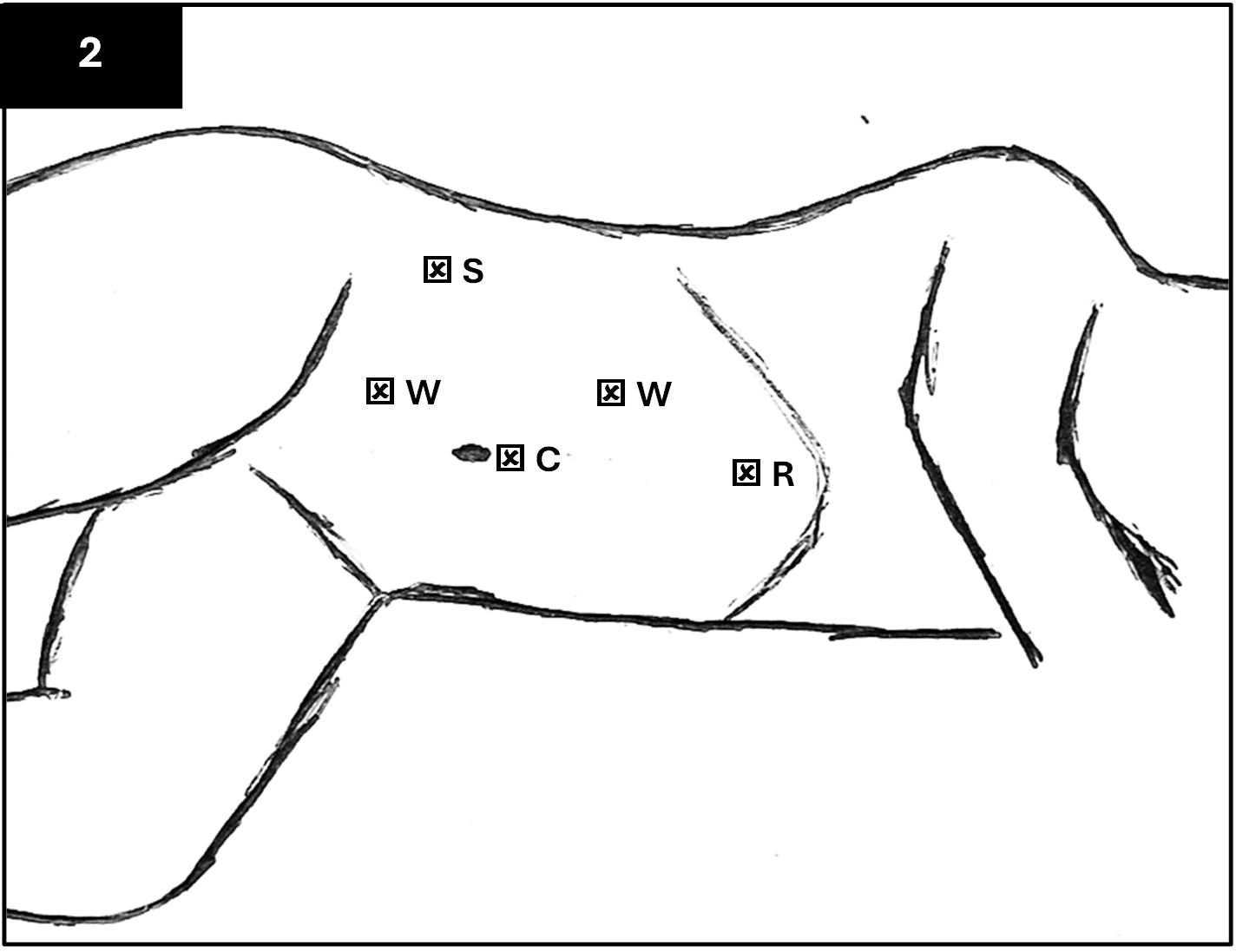
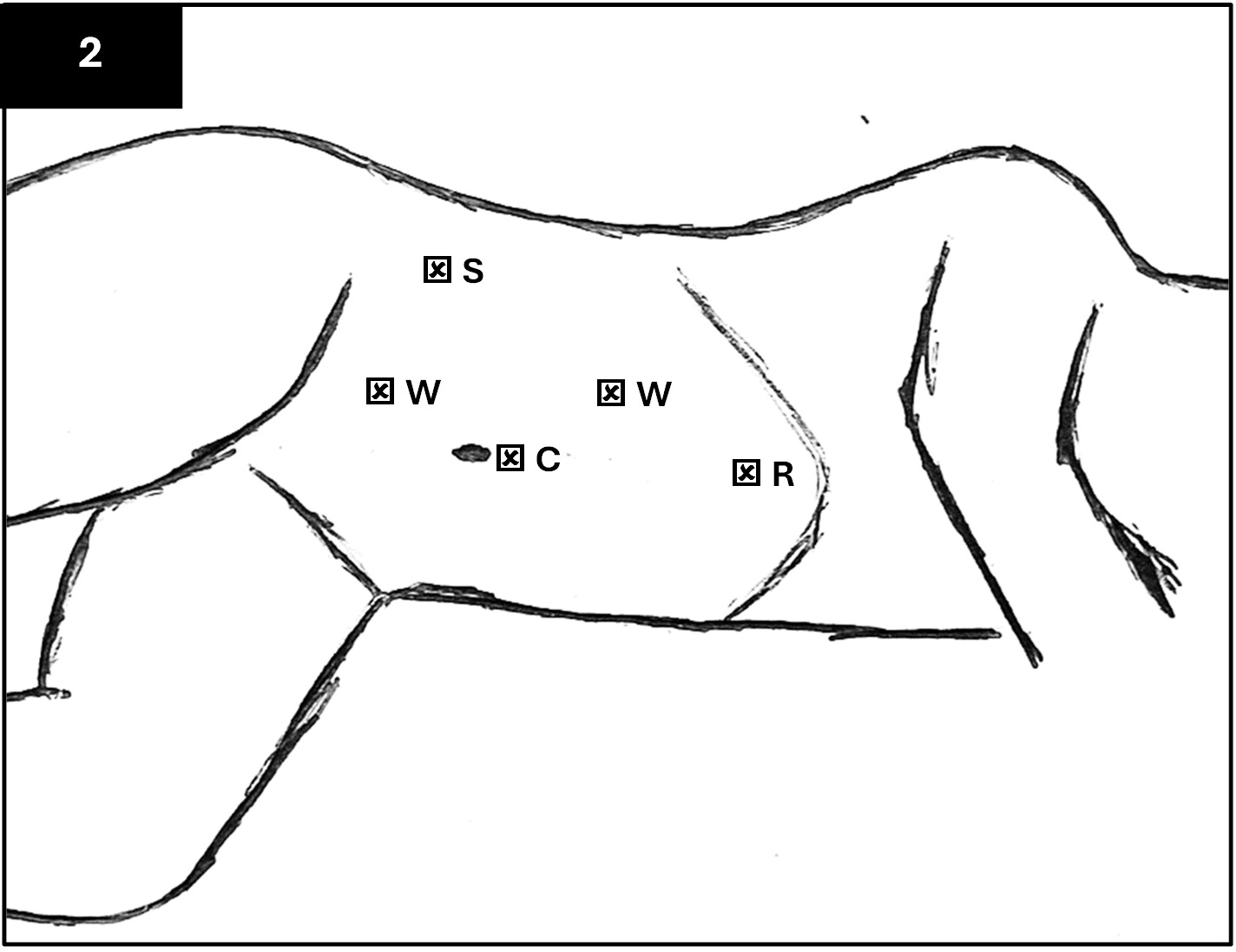
Initially, as we awaited the DTPA scan, a conservative approach was employed with pain management and adequate hydration. However, the patient continued to have worsening right-sided flank pain and an increasing level of hydronephrosis on subsequent ultrasound scans. Written informed consent was obtained for the right pyeloplasty because of worsening pain, and the patient was prepared for a right laparoscopic approach. The patient was put in the left lateral position and the laparoscopic ports were placed as shown in Figure 2.
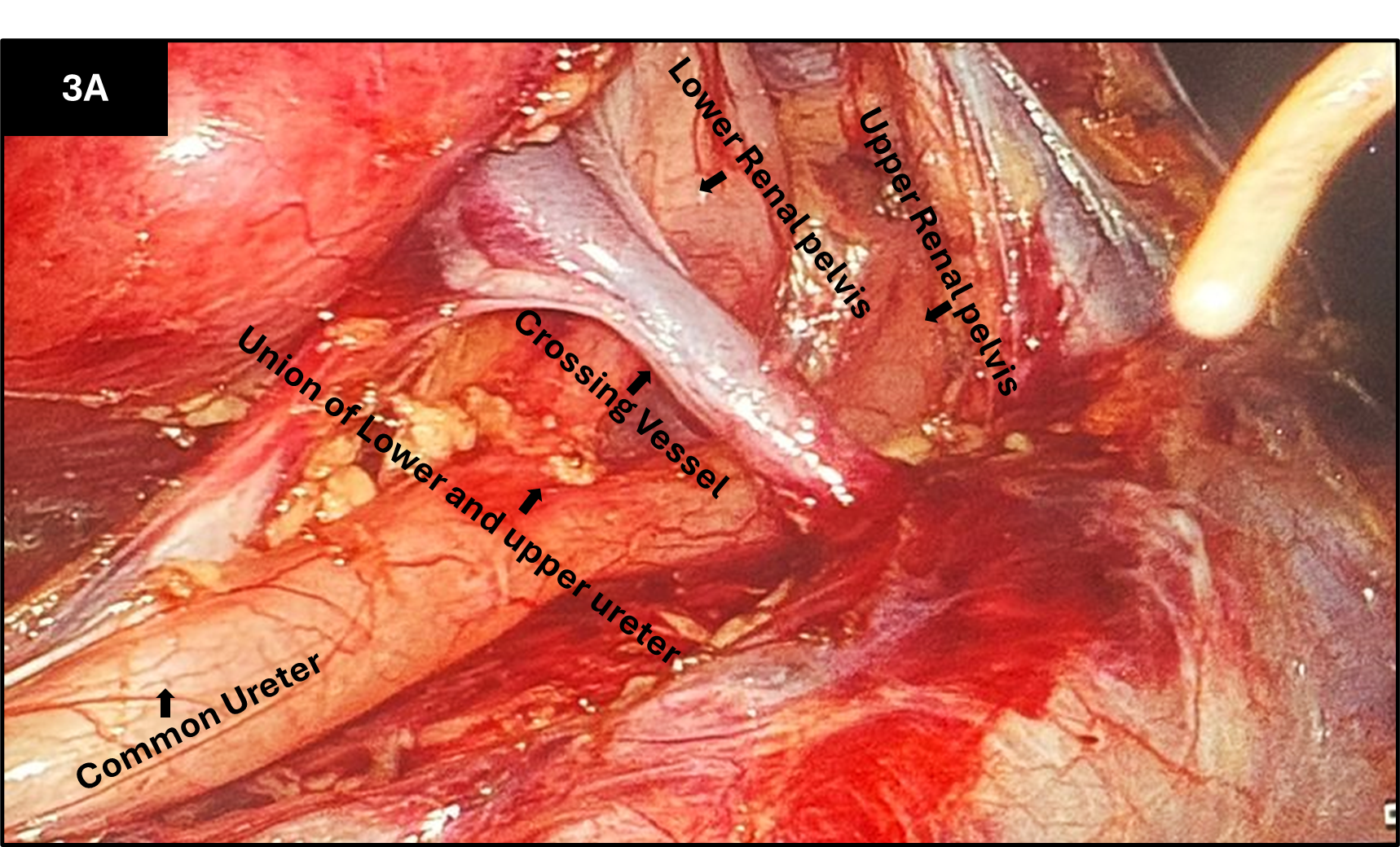
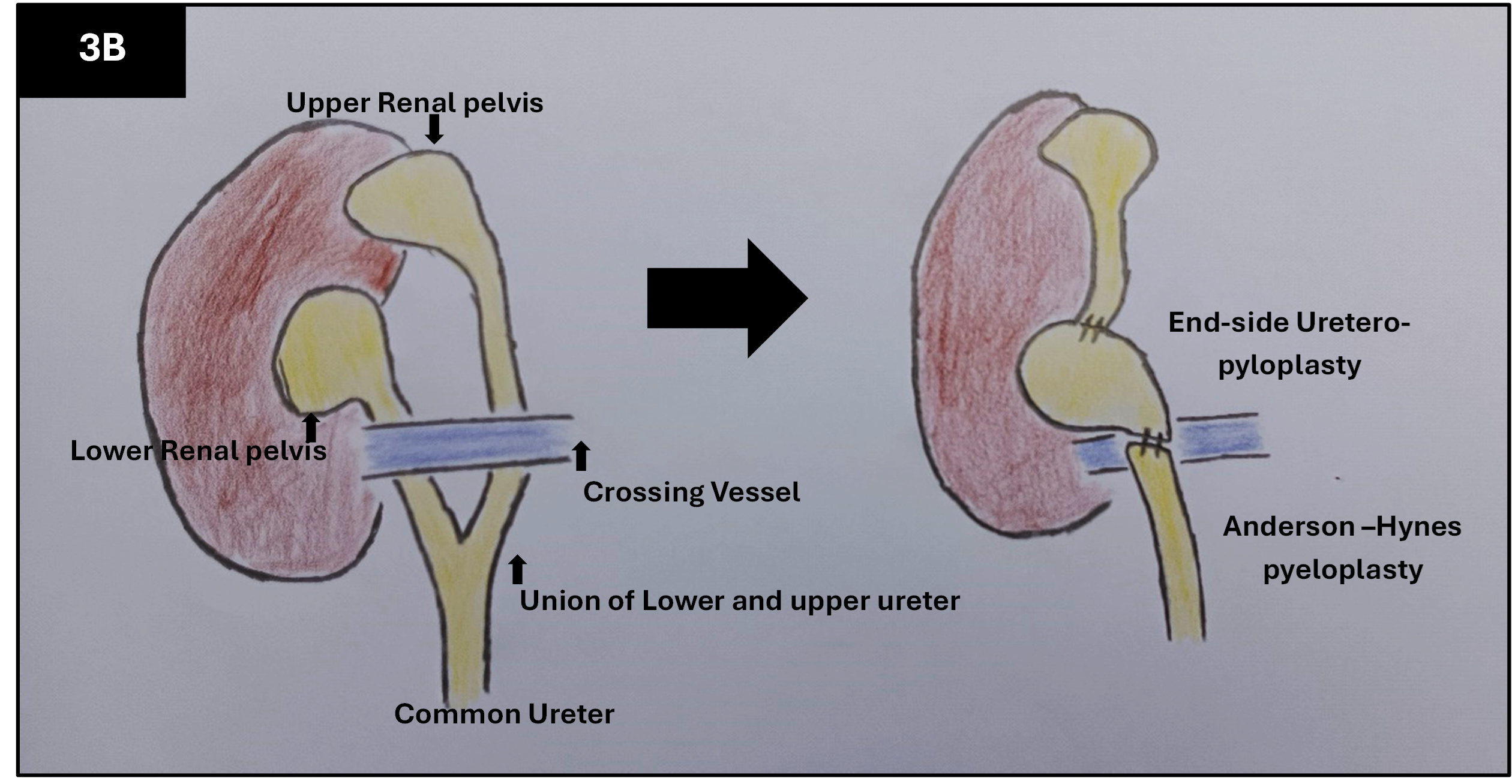
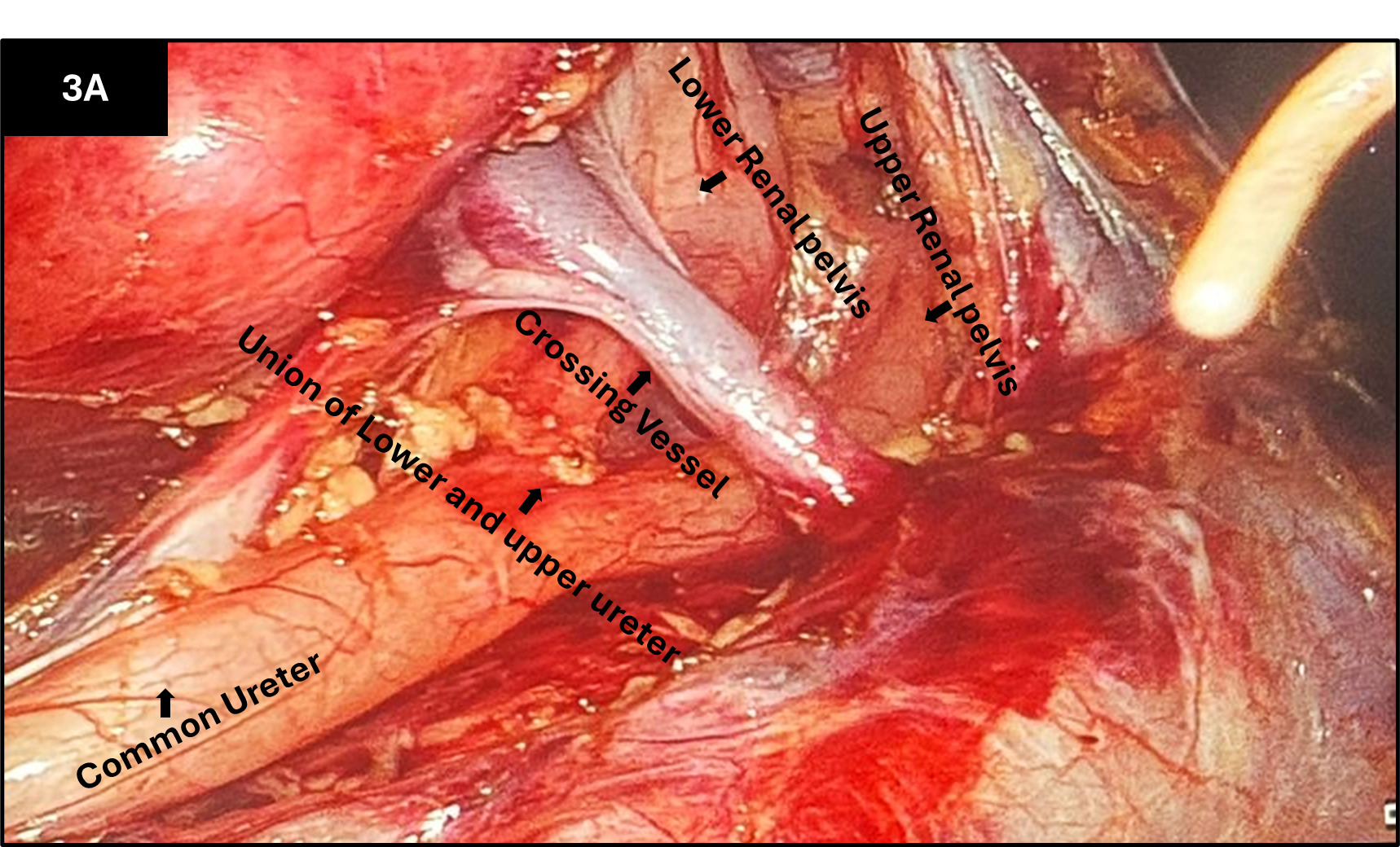
Upon exposing the right kidney, we noted an incomplete duplex system. There were 2 ureters, an upper and lower ureter, which joined to form a common ureter below the renal pelvis of the lower moiety, and a crossing vessel obstructing both upper and lower proximal ureters (Figure 3A). Dissection was done laparoscopically to expose all structures, and a stay suture was placed on the lower pelvis, which was used to exteriorize the site through a small flank incision for extracorporeal surgery. The lower ureter was dismembered from the pelvis, allowing the vessel to pass posterior to the ureter. Pyeloplasty was then performed using the standard Anderson-Hynes technique. The ureteropelvic segment was dismembered around the area of the crossing vessel on the lower pole of the ureter before anastomosing the lower pole of the pelvis to the common ureter, thereby eliminating any potential intrinsic causes of obstruction.
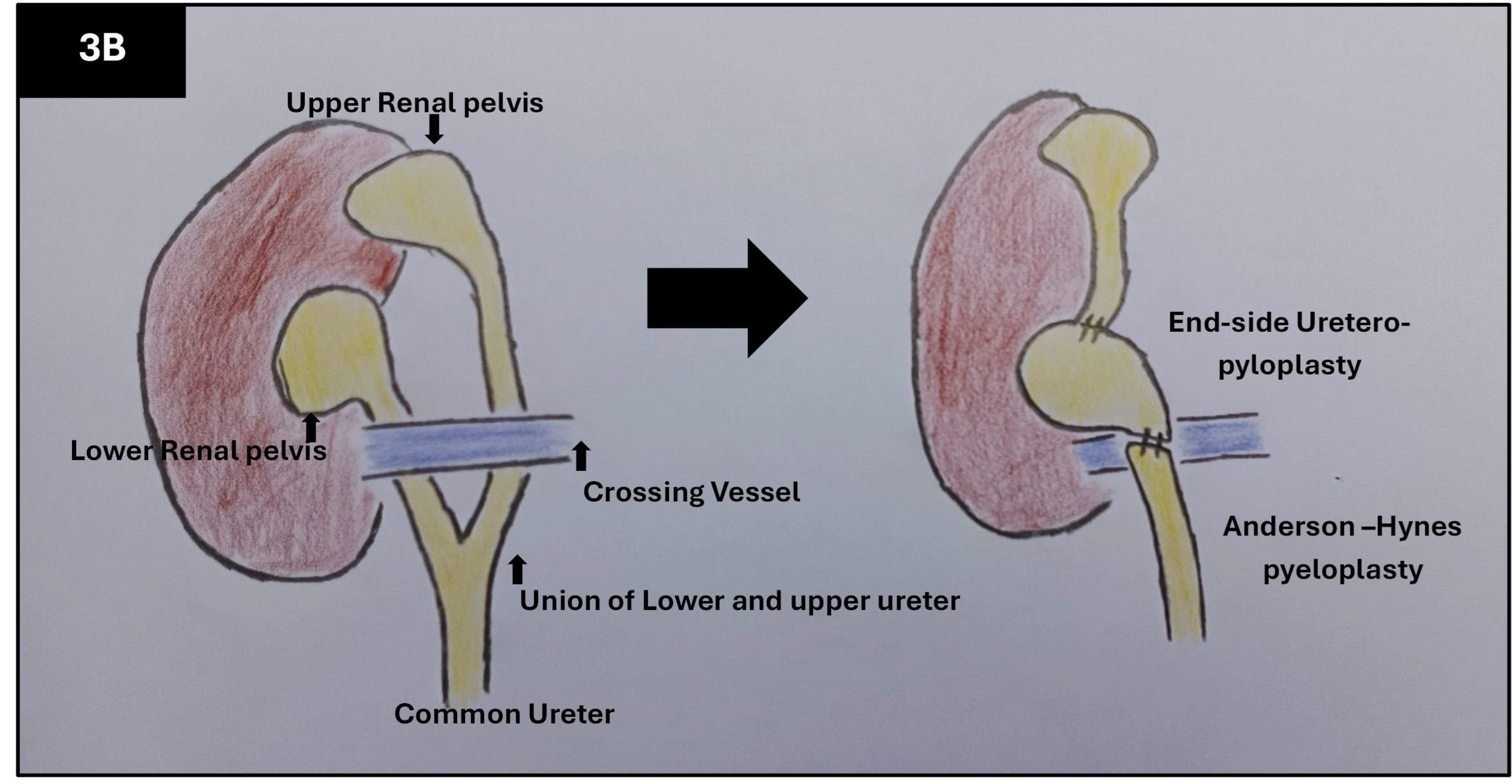
Subsequently, the upper ureter was also dismembered from its union to the common ureter, and an upper-pole ureter to lower pole pyeloplasty was performed. This way, the upper ureter drained onto the lower pelvis while the lower pelvis drained onto the common ureter (Figure 3B). The crossing vessel would now sit posteriorly to both upper and lower systems and not cause any obstruction. A double-J (DJ) stent was left in situ with the tip sitting at the lower pelvis. The total operating time was 150 minutes.
The DJ stent was removed in 6 weeks. There was a resolution of symptoms after the surgery, and an ultrasound scan done 3 months later showed a hydronephrosis of grade 1, which resolved at the 6-month follow-up scan. The patient remains on follow-up at the outpatient clinic and has reported no symptoms.
Discussion
Duplication of the collecting system can occur in complete or incomplete variants, with a reported incidence of 0.8% in the literature.3 PUJO is a rare concurrence, and when it occurs, it often affects the lower moiety in incomplete duplex systems.2 The diagnosis of this entity is challenging, given its rarity in occurrence and the nonspecific symptomatology. In our present case, the initial diagnosis of right hydronephrosis was made via ultrasonography after the patient reported experiencing right-sided flank pain for over 2 years. The duplex system on imaging may appear as 2 central echo complexes with hydronephrosis in 1 or both moieties and an intervening renal parenchyma. These findings were partially appreciated in our reported case and would have warranted further evaluation with a CT IVU, which provides superior anatomical detail and can aid in identifying potential extrinsic causes such as a crossing vessel. However, this was not performed in our case due to financial constraints, representing a study limitation.
While [99mTc]-MAG3 is the preferred tracer for obstructive kinetics due to its higher extraction fraction, [99mTc]-DTPA was used as a diagnostic alternative due to institutional unavailability. Diuretic renography and functional magnetic resonance urography (fMRU) are usually performed to detect split renal function and to assess renal clearance. In particular, the utility of fMRU is considered superior due to its ability to detect concurrent urologic pathology and vascular anatomy in addition to providing separate detail of each moiety, which are all important in surgical planning.4
The feasibility of minimally invasive techniques, including both laparoscopic and robotic options, is gaining popularity in the pediatric population. In addition to the other described benefits of shorter hospital stays, reduced pain, and excellent cosmetic outcomes, minimally invasive surgery provides excellent anatomic visualization of the duplicated system, which enhances surgical decision-making.5 These approaches can be compounded by the availability of equipment and a steep learning curve, especially on intracorporeal suturing and knotting.6 In our case, the laparoscopic-assisted approach provided a very clear description of the incomplete duplex and crossing vessel obstructing both upper and lower ureters while performing faster extracorporeal suturing.
Ueki et al describes a detailed 3-pronged approach based on intraoperative findings of the intact ureteral length and the presence of crossing vessels.7 In the absence of crossing vessels, an end-to-side pyelo-ureterostomy or an Anderson-Hynes pyeloplasty of the affected lower pole is considered. However, the presence of crossing vessels usually obstructs both ureters, and the recommended procedure is an upper-pole ureter to lower pole pelvis uretero-pyeloplasty with the Anderson-Hynes procedure for the lower pole.7 In our case, we elected to perform the latter based on the presence of a crossing vessel causing upstream dilatation in both upper and lower moieties.
In our institution, we routinely perform a DJ stented pyeloplasty as protocol in PUJO. Notably, a network meta-analysis that focused on the role of stents in pediatric pyeloplasty concluded that there were no significant differences in operative time, operative success, hospital stay, improvement of renal functions, and overall complications for the external stented, DJ stented, and stentless procedures.8
Our follow-up protocol after pyeloplasty is a clinic visit in 2 weeks, and the DJ stent is removed after 4-6 weeks. We perform an ultrasonography 6 weeks after the DJ stent removal and every 3 months thereafter. We only offer a diuretic study if there is persistent and/or increasing hydronephrosis. The follow-up protocol in the literature varies between institutions; however, the goal remains the same, which is to evaluate the adequacy of drainage and detect complications that may need intervention.9,10
Conclusion
The concurrence of PUJO and duplicated systems is a rare occurrence, and more so when associated with a crossing vessel. Surgical decision-making is based on imaging details and intraoperative dissection of the anatomic variants. When both upper and lower moieties are retained, the goal of surgery is to relieve the obstruction and ensure dependent urine flow on both moieties. The use of minimally invasive techniques is based on the availability of equipment and skill. A laparoscopic-assisted technique can be useful for beginners. This technique has the advantage of reducing operative time with extracorporeal suturing and the benefit of laparoscopic dissection, which offers adequate exposure.
Ethical Approval
Formal ethical approval was sought and granted by the Kenyatta National Hospital-University of Nairobi Ethics Review Committee (KNH/UON-ERC). Reference Number: KNH-ERC/01/PUB/3.
Informed Consent
Written informed consent for submission and publication of this case, including imaging, has been obtained from the patient. Patient privacy and confidentiality have been maintained, and all patient identifiers have been removed.
Data Availability
Not applicable.
Conflict of Interest
None
Funding
None
Acknowledgement
A preprint version of this manuscript was deposited on Research Square on 19 December 2024: Tim Jumbi, Syovata Munyalo, David Shipapa, et al. Laparoscopic-assisted approach to a right pelvi-ureteric junction obstruction with incomplete duplex system: a case report. Research Square. Preprint. https://doi.org/10.21203/rs.3.rs-5385261/v1