Introduction
Hemorrhoidal disease (HD) is the most common anorectal condition worldwide, affecting approximately 4% of the global population, with peak prevalence during the fifth to seventh decades of life. It is a clinically important disease, leading to significant workload, and is associated with significant complications if left untreated, including bleeding leading to anemia, hygiene issues, progression to prolapse, painful thrombosis, and impairment of quality of life (QoL).1–3 Patients typically present with painless rectal bleeding, prolapse, pruritus, discomfort, mucous discharge, or thrombosis. Hemorrhoids are classified as internal or external according to their origin relative to the dentate line, with internal hemorrhoids graded I–IV by the Goligher system, which remains the cornerstone of clinical assessment.4–7 In this classification, first degree remains inside the anal canal during defecation, second degree prolapses and ascends spontaneously, third degree prolapses but stays inside the anal canal on manual reduction, while fourth degree stays outside the anal canal.
Hemorrhoidal cushions are normal anatomical structures that contribute up to 15–20% of resting anal continence, and their role in fine continence control underscores the functional consequences of disease progression.8,9 Pathophysiology evolves through vascular hyperplasia, connective-tissue attenuation, venous dilation, and disruption of supporting suspensory ligaments, all of which culminate in prolapse, which is recognized as the hallmark of advanced HD.10,11 If untreated, HD may lead to chronic bleeding with anemia, painful thrombosis, hygiene impairment, and a significant reduction in QoL.
Surgery is indicated for Grade III–IV hemorrhoids and for Grade II only if disease is unresponsive to conservative therapy, as consistently emphasized across major international guidelines, including ASCRS, ESCP, SICCR, SIUCP, and Japanese guidelines.1–7 Over the past 2 decades, operative management has expanded dramatically.11–14 Traditional excisional hemorrhoidectomy, long considered the gold standard for durable control, remains widely used due to its low recurrence rates.15–18 This includes both Milligan-Morgan (the open type) and Ferguson (the closed type), in reference to the wound resulting from the hemorrhoidal excision. The conventional procedures are associated with substantial pain, delayed recovery, and increased wound-related morbidity, leading to increased popularity of minimally invasive and energy-based procedures which address patient-centered concerns such as pain intensity, early recovery, and resumption of regular activities. Energy-based devices used Bipolar diathermy, Harmonic Scalpel, and LigaSure™ hemorrhoidectomy, while other modalities include laser hemorrhoidoplasty, Doppler-guided hemorrhoidal artery ligation, and stapled hemorrhoidopexy. Meta-analyses and randomized controlled trials (RCTs) revealed lower postoperative pain scores, shorter operative times, faster recovery, lower wound-related morbidity, and lower bleeding rates with minimally invasive procedures; however, they are linked to higher recurrence rates than conventional excisional procedures.19–31
There is persistent substantial variation in the recommendation of newly introduced procedures, such as laser or energy-based procedures, despite the presence of several high-quality guidelines and consensus statements.1–8 A comprehensive appraisal of these procedures is deemed difficult due to heterogeneous study designs, inconsistent reporting of outcomes, variable anatomical complexity, and different surgeon experiences.
In the era of rapid evolution of surgical procedures addressing HD and in absence of universal guidelines, there is continuous demand for comparative updates using data from recent meta-analyses, RCTs, and large cohort studies. The aim of this systematic review is to evaluate and compare the short- and long-term outcomes of operative procedures performed for HD treatment. Additionally, it aims to produce evidence-based guidance to enhance individualized surgical decision-making.
Methods
This review followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines for evaluating existing articles and was registered in PROSPERO, the International Prospective Register of Systematic Reviews with registration number 1339929.
Search strategy
Using Medical Subject Headings (MeSH) and free-text keywords, we conducted a literature search across the major medical databases, including Embase, Google Scholar, Scopus, PubMed, and the Cochrane library. The search focused on meta-analyses, RCTs, guidelines, and major cohort studies on operative management of hemorrhoids published in the period between January 2010–December 2025. The search strategy combined Medical Subject Headings (MeSH) and free-text keywords using Boolean operators (AND, OR). The core search string used for PubMed was as follows: ((“Hemorrhoids”[Mesh] OR hemorrhoid OR haemorrhoid OR hemorrhoidal disease) AND (“Hemorrhoidectomy”[Mesh] OR hemorrhoidectomy OR excisional hemorrhoidectomy OR Milligan-Morgan OR Ferguson) OR (“Laser Therapy”[Mesh] OR laser hemorrhoidoplasty OR LHP) OR (LigaSure OR bipolar diathermy OR harmonic scalpel) OR (“Stapled Hemorrhoidopexy” OR stapled hemorrhoidopexy OR stapled hemorrhoidectomy) OR (“Hemorrhoidal Artery Ligation” OR HAL OR THD OR DGHAL OR RAR)) AND (surgery OR operative management OR postoperative outcomes OR complications OR recurrence)). The search strategy was adapted appropriately for other databases using their specific indexing terms and syntax. Reference lists of included articles and major clinical guidelines were also manually screened to identify additional relevant studies.
Study selection
Two reviewers independently screened the articles using the Rayyan screening tool. After data duplication and eligibility checks, relevant studies proceeded to a full-text review. Disagreements were resolved by consensus or by a senior reviewer’s opinion. The full texts of the selected articles were retrieved. This systematic review analyzed studies on surgical procedures for HD treatment. The types of studies included were meta-analyses, RCTs, cohort studies, and clinical guidelines on the management and outcomes of hemorrhoids published between 2010–2025.
Inclusion criteria
This systemic review included studies that highlighted the incidence of HD, assessed the postoperative outcomes of different surgical procedures performed for hemorrhoids treatment, and those that compared different surgical options.
Exclusion criteria
Excluded studies include letters to the editor, case reports, personal opinions, and studies published in non-English languages. Exclusion of case reports is justified by their limited generalizability, the absence of control comparison, and because they considered anecdotal evidence. The exclusion of non-English articles was due to difficulties in achieving accurate translations that ensured proper data extraction.
Data extraction, Quality assessment and risk of bias
The extracted data included study information, patient demographics, indications for surgery, various operative procedures, clinical outcomes, and postoperative complications. The reviewed articles were assessed for quality using relevant methods. For meta-analyses and clinical guidelines, the AMSTAR 2 (A MeaSurement Tool to Assess systematic Reviews) criteria were employed. The Cochrane Risk of Bias tool was used to evaluate Randomized Clinical Trials (RCTs), and the Newcastle-Ottawa scale was used for cohort studies.
Data synthesis and analysis
A qualitative synthesis was conducted, and the relevant findings were compiled into a narrative summary accompanied by tables and figures. Descriptive statistics were used for pooled data whenever possible. A meta-analysis was not conducted due to the heterogeneity of the articles, their varying methods, and diverse outcomes. Heterogeneity was evaluated clinically by comparing patients, disease characteristics, and postoperative outcomes. Methodological heterogeneity was assessed via differences in study design, follow-up duration, and risk of bias. Statistical heterogeneity was quantified using Cochran’s Q, I², and τ² statistics, with an I² > 50% indicating substantial heterogeneity. Where heterogeneity remained unexplained, results were summarized narratively. The qualitative analysis included the evaluation of postoperative outcomes and QoL after various surgical procedures.
Results
Study selection and characteristics
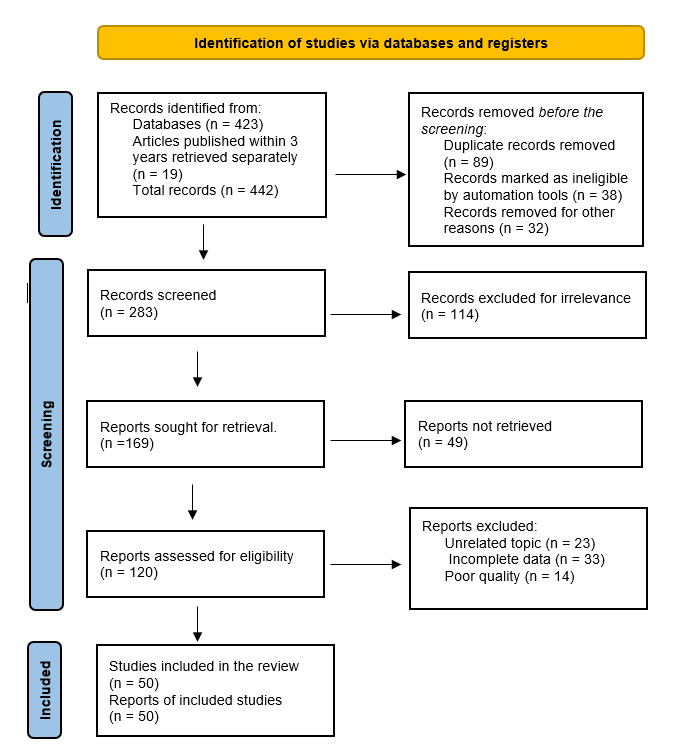
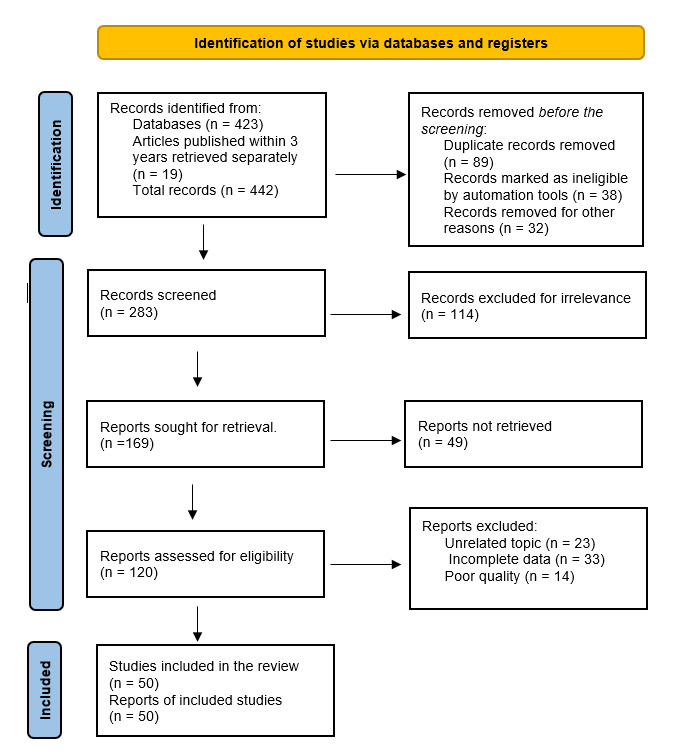
As illustrated in Figure 1, a total of 423 articles were retrieved from the initial search across the electronic databases. To ensure contemporary evidence coverage, 19 additional recent studies from the past 3 years were manually added. A total of 283 articles underwent title and abstract screening after removing 70 articles by automation, for different reasons, and removing 89 duplicates. Another 114 reports were removed due to irrelevance, inadequate methodological quality, or because they were in a non-English language. The planned number for retrieval was 169, but the actual number was 120 full-text articles, which were all assessed for eligibility. An additional 70 articles were excluded due to methodological issues or because they failed to meet inclusion criteria. The final number included in the review was 50 studies, including RCTs, systematic reviews, meta-analyses, observational cohort studies, and major international clinical guidelines or consensus statements focusing on evaluation of operative management of hemorrhoids (Table 1). The methodological quality and risk of bias of the included studies were assessed using design-appropriate tools, including AGREE II for guidelines, AMSTAR 2 for systematic reviews, the Cochrane Risk of Bias tool for randomized trials, and the Newcastle–Ottawa Scale/ROBINS-I framework for observational studies. The detailed assessment is presented in the supplementary files (Tables A1–A4). Overall, randomized controlled trials demonstrated low to moderate risk of bias, mainly related to the unavoidable lack of blinding in surgical trials. Observational studies generally showed moderate risk of bias, primarily due to selection bias and residual confounding. Systematic reviews included in this analysis demonstrated moderate-to-low risk of bias, while international guidelines showed high methodological quality according to AGREE II appraisal. The range of sample sizes across the studies was from 40–666 participants, and follow-up durations were from 3 months to 15 years, providing robust evidence on both short- and long-term outcomes across all major surgical modalities. This wide range enabled a comprehensive comparative assessment of outcomes of different operative procedures for managing advanced HD (Tables 2–6).
Postoperative pain
Postoperative pain scores are directly proportional to the extent of tissue disruption, the volume excised, and wound size, resulting in variable pain intensity across operative modalities. The highest early postoperative pain scores were documented with conventional excisional hemorrhoidectomy (Milligan-Morgan and Ferguson) in several RCTs and metanalyzes, with day-1 VAS scores commonly between 6–9.15–18 In the early postoperative period (5–8 days) pain frequently persisted at significant levels, which is attributed to the extensive open wound in the highly innervated anoderm, leading to elevated analgesic needs. Energy-based excisional procedures significantly reduced pain intensity, improving the clinical outcomes. Several RCTs demonstrated that LigaSure™ hemorrhoidectomy reduced pain intensity by 30–45% compared to MMH, while Harmonic Scalpel and Bipolar diathermy procedures demonstrated significant reduction of day-1 VAS values down to 3–5. This was attributed to reduced stimulation of ano-cutaneous nociceptors, leading to lower analgesic requirements.19–23
The most favorable pain profile was demonstrated with laser hemorrhoidoplasty (LHP) with day-1 VAS scores ranged from 2–4, with reduced analgesic requirement in day 3–5 postoperatively. This is attributed to the absence of excision and minimal neuronal injury associated with its submucosal photothermal mechanism.24–29 Doppler-guided hemorrhoidal artery ligation procedures (HAL/DGHAL/HAL-RAR) are linked to lower early pain scores, typically 2–5 at 24 hours, due to the preservation of anodermal integrity.30–32,40 When compared to MMH, Stapled hemorrhoidopexy (SH) consistently provided 50–70% reduction in pain intensity in the early postoperative period,33,41,42 although staple-line tension or local ischemia, if occurred, will increase pain scores around day 3 postoperatively.
Postoperative bleeding
Risks and rates of intraoperative or postoperative bleeding rates vary significantly across operative modalities. The highest rates of bleeding occurred with conventional excisional hemorrhoidectomy, typically ranging from 1.5%–7%; however, on most occasions it is minimal and was self-limiting, rarely required surgical intervention or transfusion.15–18 Excisional procedures using energy-based devices including LigaSure™, Harmonic Scalpel, and Bipolar diathermy showed consistent superior hemostasis. Therefore, bleeding rates frequently remained low at 1–2%, reflecting precise thermal sealing and controlled dissection planes.19–23
LHP has the lowest bleeding incidence across several studies, with rates consistently below 1%, attributable to the photocoagulative closure of submucosal vascular channels and the absence of an open wound surface.24–29 Despite this, SH demonstrated minor bleeding and low incidence bleeding rates of 2–5%; however, rare cases of severe staple-line hemorrhage require endoscopic or operative management.41,42 Similarly low rates around 2–5% were documented after HAL/DGHAL and HAL-RAR, which were minimal and managed conservatively in most cases.30–32,40
Complications
Complication profiles are reflections of the expected gradient of procedural invasiveness. Conventional excisional hemorrhoidectomy was known for the highest postoperative morbidities, including urinary retention (3–15%), wound infection (2–6%), delayed wound healing (up to 10%), and anal stenosis (2–3%).15–18 These outcomes are attributed to large open wound size and extensive tissue disruption. Low rates of postoperative complications were observed with energy-based excisional techniques, attributable to minimized tissue trauma, improved thermal precision, and faster epithelialization. Rarely, major complications such as stenosis or incontinence were detected at a very low rate of 1–2%.19–23
SH is associated with a distinct profile of unique complications, such as pelvic sepsis, chronic urgency, staple-line dehiscence, and rare rectal or mesorectal prolapse. Rare but very serious complications in these events were demonstrated in several RCTs with long follow-up durations.33,34,41,42 The most favorable safety profile was linked to minimally invasive modalities with minor complications such as local edema, mild thrombosis, and temporary discomfort.24–32,40 HAL-RAR may lead to residual skin tags and persistent prolapse in patients presented with a large external component of hemorrhoids with insufficient mucopexy or plication. Advanced grades of hemorrhoids, inadequate anatomical correction, and technical factors lead to late complications such as chronic pain, incontinence, recurrence, or anal stenosis.43,44
Recurrence
The incidence of recurrence is significantly influenced by the degree of anatomic correction, which varies considerably across different procedures. The lowest recurrence rates were observed with excisional hemorrhoidectomy at 0–3% at 12 months, across multiple high-quality studies.15–18 Energy-based excisional modalities including LigaSure™ and Harmonic Scalpel showed similarly low recurrence rates of 1–4%.19–23
SH showed a biphasic pattern in recurrences as a moderate recurrence, ranging from 6–12% in short-term follow-ups; however, with long-term follow-up studies revealed escalating recurrence rates up to 47%, particularly in patients with large external components or significant mucosal redundancy.33,34,41,42
Higher recurrence rates were demonstrated with minimally invasive procedures. LHP showed 3–8% recurrence rate in Grade II–III hemorrhoids and 12–20% in Grade IV, while HAL/DGHAL/HAL-RAR show recurrence in 8–20%. The incidence here is strongly dependent on anatomical complexity and surgeon experience. These patterns were consistently reported across RCTs, cohort studies, and meta-analyses.24–32,35,36,40,43,44
Operative time
Operative time duration was affected by steps of procedures and surgeon experience. The longest duration was observed with open excisional hemorrhoidectomy (MMH/FH), requiring 25–40 minutes, although the duration depends on number of removed columns.15–18 LHP, LigaSure™, and Harmonic Scalpel techniques have almost comparable average operative times of 15–25 minutes, reflecting rapid dissection and efficient hemostasis.19–29 HAL/DGHAL and HAL-RAR procedures have an average operative time of 20–30 minutes, with longer durations required for mucopexy.30–32,40 The shortest operative duration was observed for SH, with a range of 10–20 minutes.41,42
Recovery and return to normal activity
Recovery time is directly proportional to the intensity of postoperative pain, the volume of tissue disruption, and wound size. The slowest recovery was observed in patients who underwent excisional hemorrhoidectomy (MMH/FH), requiring 3–4 weeks to resume normal activities.15–18 Energy-based hemorrhoidectomies are associated with early mobilization and shorter recovery time, with a range of 10–14 days due to less pain, as has been demonstrated in several RCTs.19–23 The fastest recovery was observed with LHP, with resumption of regular daily activities within 5–10 days.24–29 Recovery was achieved within 7–12 days with HAL/DGHAL/HAL-RAR, while SH typically permitted activity within 10–14 days.30–34,40–42
Quality of life
Obviously, QoL has significantly improved with the new, minimally invasive operative procedures. Validated protocols and instruments including WHOQOL-BREF, EQ-5D, HSS, and HEMO-QoL, were used in different studies reporting rapid early QoL improvement after LHP and HAL/DGHAL because of minimal pain, while the most durable long-term QoL was after excisional hemorrhoidectomy due to low recurrence.35–37,43–47 Both short- and long-term QoL outcomes are influenced by patients’ perception to patterns of pain, recovery time, and recurrence.
Length of hospital stay
Length of stay is determined by wound recovery, which is inversely proportional to the invasiveness of the procedure. Conventional hemorrhoidectomy (MMH/FH) will stay for 1–4 days.15–18 For the daycare procedures or same day surgical procedures such as LigaSure™, Harmonic Scalpel,19–23 laser hemorrhoidoplasty, HAL/DGHAL, and HAL-RAR,24–32,40 patients will nearly be discharged in the same day. and a SH will need >24 hours observation.33,34,41,42
Discussion
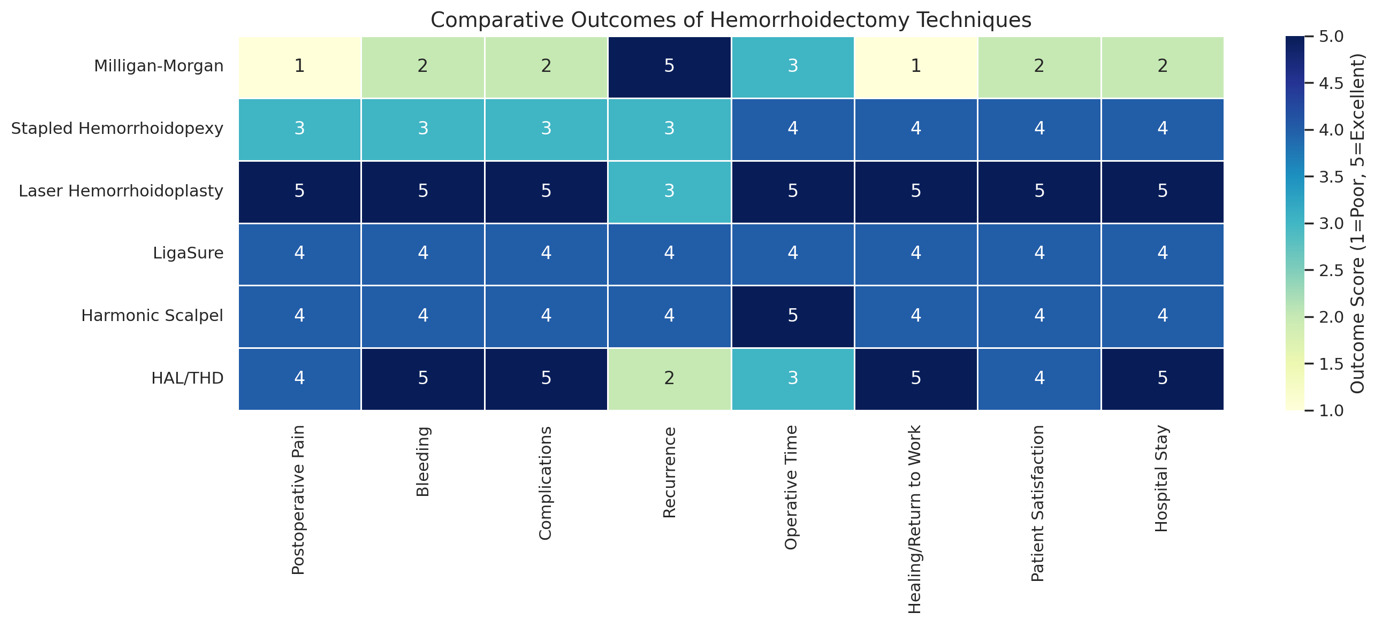
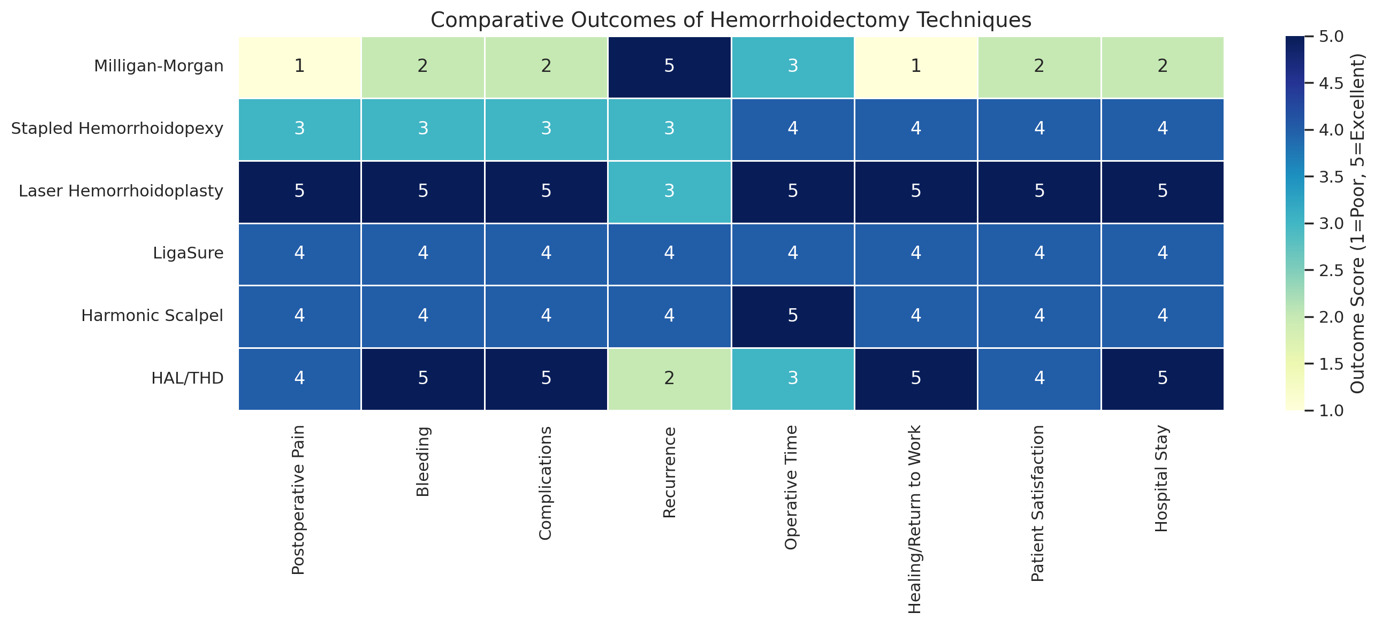
This review studied 50 articles demonstrating substantial heterogeneity in outcomes among operative modalities performed for hemorrhoid treatment. The findings demonstrated that there is not a single universally superior procedure. Each procedure provides a different balance of outcomes, including pain reduction, hemostasis, complication risk, recurrence, and functional recovery. The variable outcomes are attributable to different degrees of tissue disruption, vascular control, anatomical preservation, and energy delivery mechanisms inherent to each technique.1–10 Figure 2 shows different outcomes with variable modalities.
Postoperative pain: The central determinant of patient recovery
Postoperative pain associated with operative modalities treating HD is the most influential outcome and is one of the strongest predictors of delayed resumption of regular activities and reduced early QoL. The highest pain scores were observed with conventional excisional hemorrhoidectomy (MMH/FH), which was the main drive for evolution in operative procedures that produce less pain. This was demonstrated across several studies, guidelines from ASCRS, ESCP, SICCR, Japanese, and SIUCP societies.1–8 Multiple RCTs revealed that day-1 VAS scores of 6–9 are attributable to intense stimulation of the highly innervated anoderm and extensive tissue dissection.9–12
Energy-based excisional procedures have reduced post-hemorrhoidectomy pain intensity by 30–45% when compared to MMH, due to improved thermal precision, less traction injury, and shorter coagulation times.11,15,17,20 Reduced analgesics requirements and improved early comfort were demonstrated in multiple meta-analyses approving these advantages.12,19,20 The lowest pain scores were demonstrated with LHP, often achieving VAS 2–4 on the first postoperative day, which is attributable to its submucosal photothermal delivery, absence of anodermal incision, and minimal inflammatory response, making this modality superior to other procedures as shown in high-quality studies.15–18,21–23 Favorable pain scores were demonstrated with Doppler-guided arterial ligation (HAL/DGHAL) and recto-anal repair (RAR) due to the absence of tissue resection altogether, a finding well-demonstrated in guidelines and multiple RCTs.24–27 SH achieves 50–70% of pain reduction compared to conventional excision in early postoperative days.13,14,28
The critical determinant predictor of postoperative pain is the extent of tissue disruption; therefore, minimally invasive modalities consistently provide early comfort and faster recovery.
Postoperative bleeding: Impact of hemostasis and energy technology
Bleeding risk depends on the volume of tissue excised, the extent of dissection, wound size, and method of hemostasis. Conventional excisional techniques (MMH/FH) are associated with the highest bleeding rate (1.5–7%), mainly attributed to wide, raw surfaces and handling of the vascular hemorrhoidal plexus.9–12,14 A bleeding rate of <2% is demonstrated with energy-based procedures due to precise dissection and effective hemostasis using LigaSure™, Harmonic Scalpel, and BDH. This was shown to be consistent across RCTs and meta-analyses reflecting less thermal damage and reliable vessel sealing.11,15,17,19,20
Several systematic reviews and large cohort studies demonstrated that precise submucosal coagulation with minimal disruption of mucosal integrity enabled LHP to produce the lowest bleeding rates (<1%).16–18,21–23,29–31 SH is associated with low bleeding rates (2–5%), but in rare incidents, severe staple-line bleeding requiring re-intervention has been documented in long-term RCTs.13,14,40 Minimal bleeding occurs in 2–5% of HAL/DGHAL and RAR cases, typically managed conservatively.24–27
Complications: Safety profiles reflect invasiveness and technique
The incidence of complications depends on wound size, anatomical distortion, and volume of excised tissues. The highest morbidity rates were linked to excisional hemorrhoidectomy, including urinary retention (3–15%), wound infection (2–6%), delayed epithelialization (up to 10%), and anal stenosis (2–3%), which were demonstrated in several studies across the review.1–4,9–12,14,32 Energy-based excisional hemorrhoidectomy is associated with lower morbidity rates than conventional procedures. This is attributable to precise dissection, superior hemostasis, and reduced collateral damage, keeping the significant complications such as stenosis and incontinence at 1–2%.11,15,17,19,20,32,41,42
SH is characterized by comfortable early postoperative recovery. However, it can give rise to unique and occasionally severe complications, such as pelvic sepsis, staple-line dehiscence, chronic urgency, rectal or mesorectal prolapse, and rare rectovaginal or rectourethral fistulas. These rare, serious complications were demonstrated across large cohort studies and RCTs with more than 15 years follow-up.13,14,28,33,34,40
Non-excisional, minimally invasive modalities demonstrated the safest profile, with transient minimal complications including recurrence of symptoms, local edema, thrombosis, persistent prolapse, or skin tags.16–18,21–27,29–31
All operative modalities, to a variable degree, can lead to long-term complications including recurrence, chronic pain, incontinence, and anal stenosis; however, these complications were most strongly correlated with disease severity, anatomical complexity, and the adequacy of prolapse correction.29,32,35,43,44
Recurrence: A trade-off between comfort and long-term durability
Recurrence rates are significantly influenced by the mechanism of tissue management. Conventional excisional hemorrhoidectomy (MMH/FH) has the lowest recurrence rates (0–3%), leading to its classification as the most durable procedure as demonstrated in guidelines, long-term cohorts, and RCTs.1–4,9–12,14,32,36 Similarly low recurrence rates (1-4%) were demonstrated with energy-based excisional modalities, supported by long-term data from large LigaSure™ and Harmonic cohorts.11,15,17,19,20,32,36,45,46 SH demonstrated moderate early recurrence (6–12%), which escalates on prolonged follow-ups reporting recurrence reaching up to 47%, especially in patients with advanced grades of hemorrhoids.13,14,28,33,34,40 The highest recurrence rates were observed with minimally invasive procedures. Recurrence rates were 3–8% in Grades II–III, rising to 12–20% in Grade IV after LHP.6–18,21–23,29–31 The range after HAL/DGHAL/RAR was 8–20%, which is significantly influenced by the anatomical distortion of hemorrhoids and surgeon expertise.24–27,35,43,44 Multiple meta-analyses demonstrated similar pattern of recurrences, emphasizing a durability-comfort trade-off across operative procedures in treatment of HD.9–11,28
Functional recovery and QoL
Functional recovery is strongly influenced by the magnitude of postoperative pain, time for wound healing, and resumption of regular activities. Conventional excisional modalities are linked to the longest recovery (3–4 weeks),9–12,14 which is attributable to the larger wounds and slower tissue regeneration, while energy-based excisional surgery allowed return to work in less than 2 weeks.11,15,17,19 Minimally invasive modalities offered the fastest recovery, as LHP patients needed 5–10 days,16–18,21–23,29–31 HAL/DGHAL needed 7–12 days,24–27 and SH needed 10–14 days for full recovery and resumption of daily activities.13,14,28,33
On applying QoL assessment tools such as WHOQOL-BREF, EQ-5D, HSS, and HEMO-QoL, consistent improvements were observed with rapid early gains following LHP and HAL, while more durable, long-term QoL benefits were observed after excisional surgery due to minimal recurrence.29,32,35,37,43,44,47 These findings were further supported by QoL validation studies and symptom-specific scoring systems.37,38,47
Alignment with ERAS principles and modern surgical priorities
Minimally invasive and energy-based modalities are the optimal option conforming with ERAS protocols because they produce lower postoperative pain scores, reduce opioid requirement, and secure hemostasis, leading to early recovery and mobilization and suiting daycare service. These observations echo the ERAS-aligned outcomes of energy-based hemorrhoidectomy, LHP, and HAL modalities.16–18,21–27,29–31,39,48
The conventional procedures (MMH/FH) are recognized as providing unmatched long-term durability, however, they are less compatible with ERAS pathway due to high pain scores in the early postoperative period, prolonged hospital stays, and longer times to functional recovery.9–12,14 Evolving pain control strategies may provide the needful support to ERAS strategies in post-hemorrhoidectomy care.49,50
Limitations
The major limitations were heterogeneity in study design, variable outcome definitions, variation in follow-up duration, and lack of high-quality RCTs for some innovative modalities such as laser and Doppler-guided techniques. Meta-analysis was not feasible. Potential publication bias may favor newer technologies.
Conclusion
There is no universally best surgical technique that suits everyone in hemorrhoid treatment; each has distinct advantages and limitations. Conventional excisional procedures have the lowest recurrence rates, with advanced grades; however, they are associated with high pain scores, complications, and delayed recovery. Minimally invasive options, such as LHP and LigaSure, have excellent early outcomes, with low pain scores and a speedy recovery, making them ideal for selected cases, particularly those with Grades II–III. Options like SH, HAL (Doppler-guided) techniques, and Harmonic Scalpel provide additional choices, balancing comfort and effectiveness. The procedure selection should be tailored to the hemorrhoid grade, patient preferences, comorbidities, and the surgeon’s expertise.
Funding
No funding.
Conflicts of Interest
The authors declare no conflicts of interest.
Ethical Approval
Ethical approval is not required for this review
Informed Consent
Not applicable
Data Availability
All data generated or analyzed during this study are included in this published article and its protocol as registered on PROSPERO [ID: 1339929].