

Introduction
The pedicled hypogastric flap has long been used as a workhorse for resurfacing large soft tissue defects of the hand.1 Its reliability, minimal donor site morbidity, and ease of execution have endeared it to reconstructive surgeons. Although, in this era of free tissue transfer, the disadvantage of 2–3 weeks of hand-groin synechiae is being obviated by an appropriately chosen free flap in facilities where such a flap is available.2,3 However, pedicled hypogastric flap use remains relevant in small children and specific clinical scenarios, especially in low-resource settings without microsurgical facilities.4,5 Various modifications of the flap to broaden its use have been described in the literature.6–8 A recent modification is the pedicled split hypogastric flap, which allows the flap to cover 2 non-contiguous hand defects or coexisting dorsal and palmar defects, thereby precluding the need for a second flap.9 This innovation reduces operating time and patient discomfort and spares another flap territory.
Since its introduction into the surgical armamentarium for hand reconstruction about 5 years ago by Sabapathy et al, there has been a lack of reports concerning outcomes in sub-Saharan Africa. This may be due to infrequently encountered indications for its use or to the availability of other, more familiar, alternatives for reconstructive surgeons. In its design, the pedicled split hypogastric flap follows the standard markings and dimensions of the hypogastric flap in the lower abdomen,2 with the only difference being the dualization of the distal flap segment after elevation. The splitting allows this single flap to effectively cover defects that would otherwise require dual-flap coverage. We hereby share our illustrative experience with the pedicled split hypogastric flap in 2 clinical scenarios and hope this will enrich the literature on its use and help lighten the burden of hand reconstruction in sub-Saharan Africa.
Case Presentation
Case 1
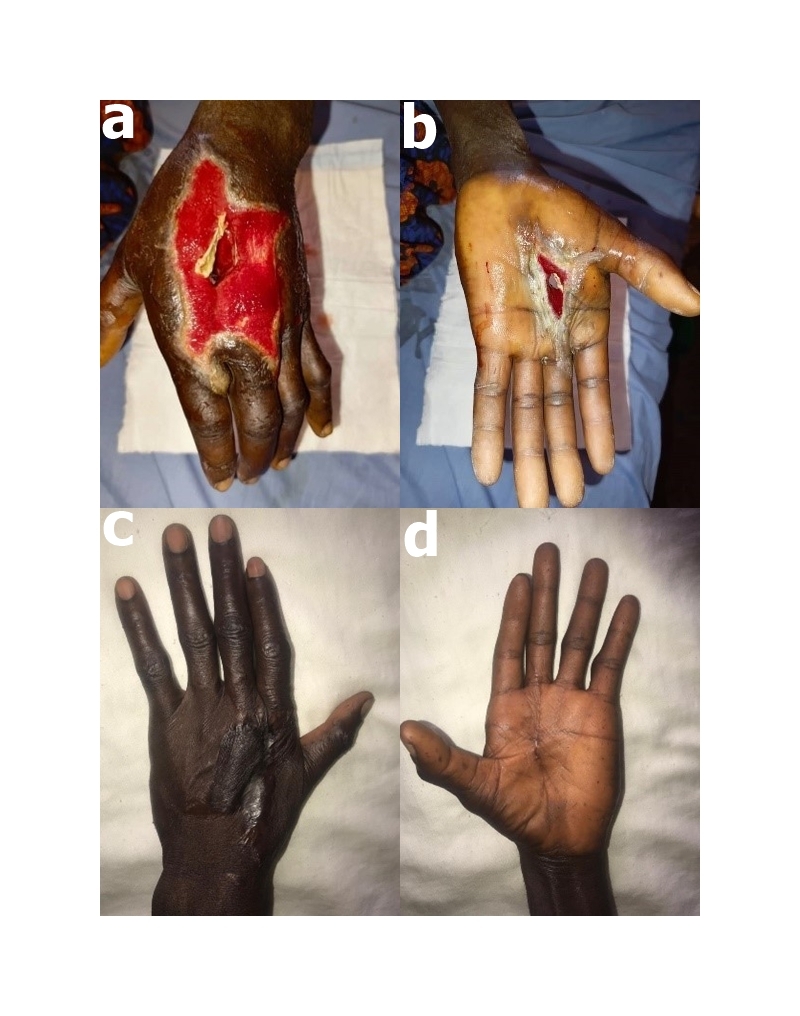
A 35-year-old right-handed man sustained a gunshot injury to the left hand while preparing his locally made Dane gun for a hunting expedition. He inadvertently pulled the trigger while his left hand covered the barrel outlet. The patient had initial resuscitation at a peripheral hospital before presenting at our institution 8 hours after the injury. Examination revealed a perforating through-and-through wound on his left hand. The smaller entry wound (4 × 7 cm) on the palm communicated with the larger dorsal exit wound (10 × 8 cm), with ragged edges (Figure 1A and B). There were necrotic and devitalized extensor tendons and soft tissues within the wound. There was also dark staining of the wound cavity from the expelled gunpowder. Deformity of the ulnar side of the patient’s hand was noted, with restricted active and passive movement. All his fingers were pink with good capillary refill.
_palmar_entry_wound_following_accidental_blast_injury_at_operative_debridement__(b)_dor.jpeg)
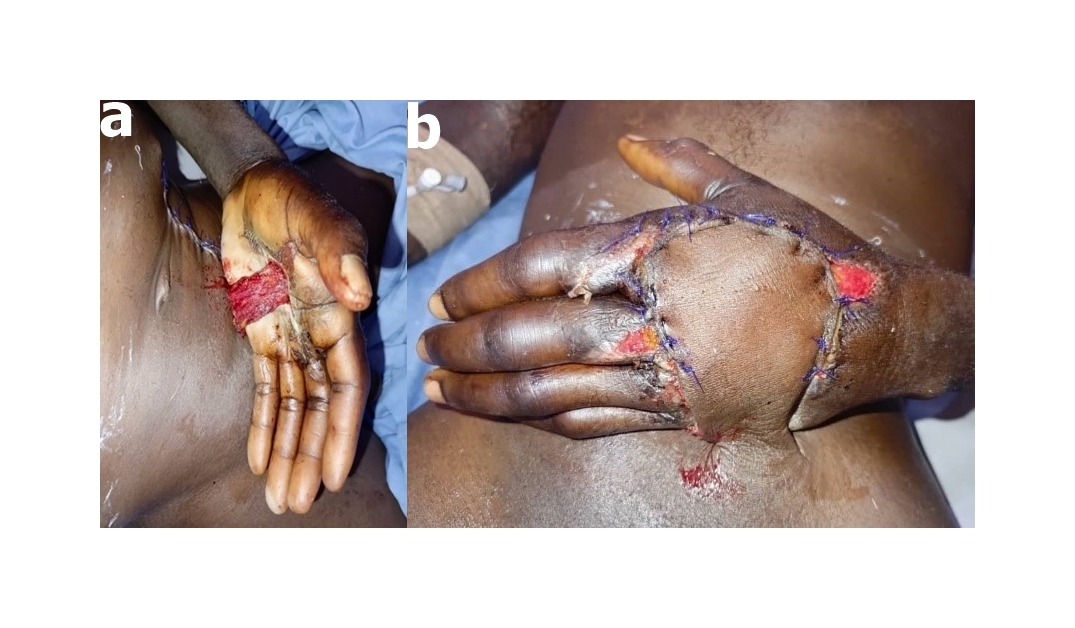
Plain radiograph revealed a midshaft fracture of the fifth metacarpal (Figure 1C). He had tetanus prophylaxis, intravenous antibiotics, analgesia, and operative wound debridement under general anesthesia. The patient’s hand was stabilized in a volar slab and subsequently received regular wound dressings and gentle physiotherapy. Soft tissue coverage was achieved with a pedicled split hypogastric flap designed on the left lower abdomen (Figure 1D). The procedure was planned for 48 hours after injury but was performed 2 weeks after injury due to logistical impediments (Figure 2A–D). The adipofascial component was used to fill the cavitary defect from the palmar side, while the cutaneous component was used to resurface the dorsal defect (Figure 3A and B). The patient developed flap-tip necrosis postoperatively, which was managed conservatively. Flap division was performed on postoperative day 21, with glabrous skin grafting over the adipofascial flap component. Graft take and donor site healing occurred uneventfully, and the patient was discharged home 2 weeks after skin grafting. He did not attend the follow-up visits; therefore, a 1-year postoperative photograph (Figure 2C and D) and a general clinical assessment were obtained during a home visit. He achieved acceptable clinical recovery and fully resumed his daily activities.
_dorsum_of_the_hand__pre-_pedicled_split_hypogastric_flap_cover__(b)_volar_surface_pre-.jpeg)
_adipofascial_flap_component_in-situ_and_(b)_cutaneous_flap_component_in_situ.jpeg)
Case 2
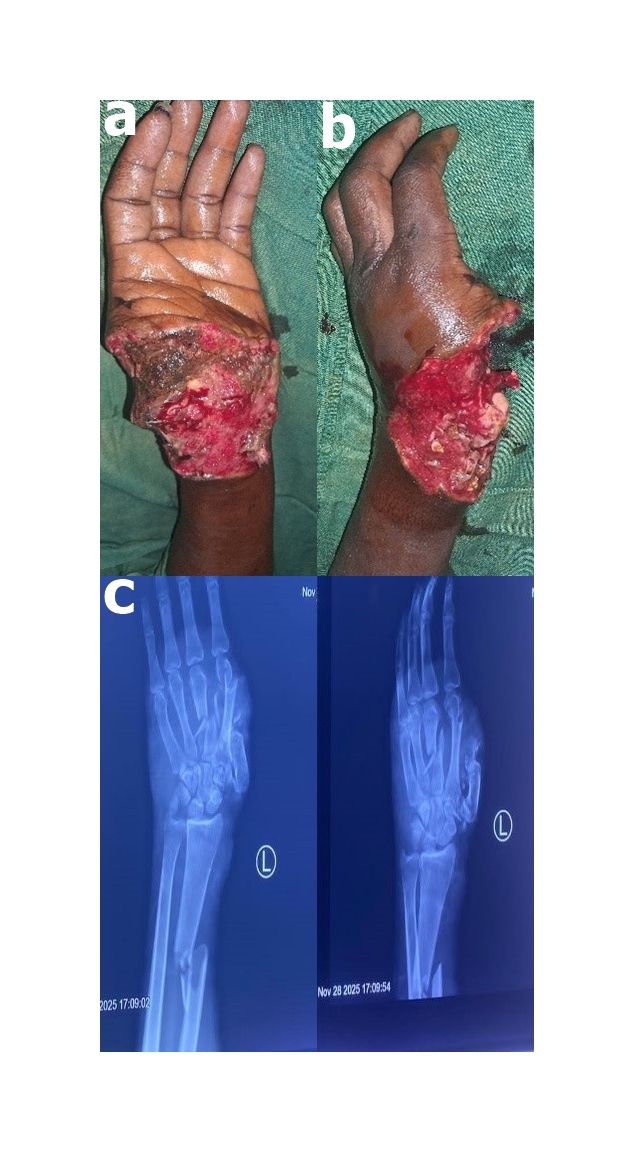
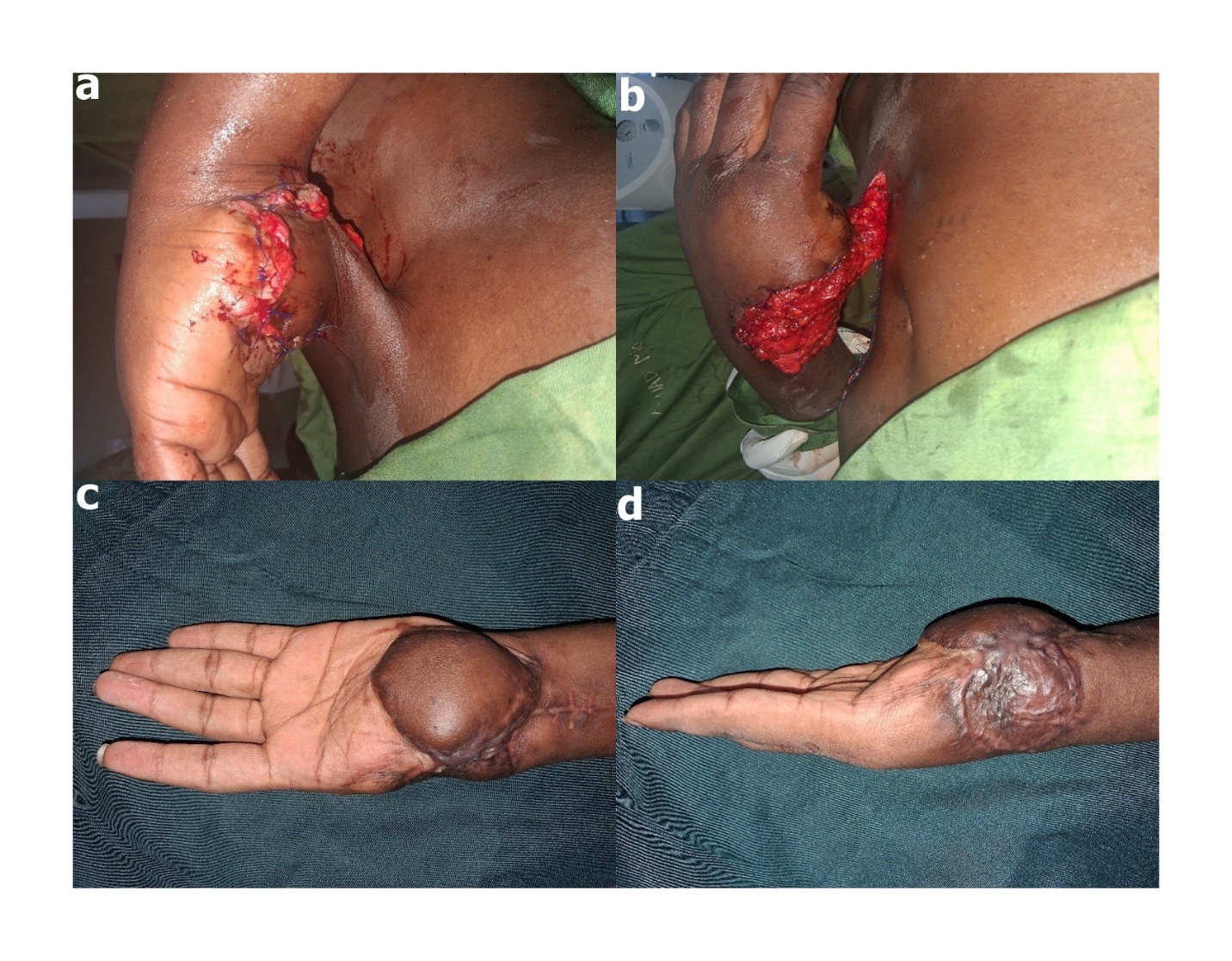
A 27-year-old right-handed man sustained a blast injury to the left hand from a sudden gas explosion while trying to repair the cork of a nitrous oxide cylinder used for filling balloons at a party. He had an initial treatment at a peripheral hospital before being referred to our institution 48 hours after the injury. Examination revealed a deformed left hand with an absent thumb and extensive soft tissue loss spanning the volar distal forearm to the proximal palmar crease and extending to the adjoining radial side of the dorsum of the hand (Figure 4A and B). There was a disarticulated first metacarpal, fractures of the second and third metacarpals, loss of the trapezium bone and thumb phalanges, a comminuted fracture of the trapezoid bone, and a displaced distal third fracture of the radius on plain radiograph (Figure 4C). The patient had extensive wound debridement done under general anesthesia and resurfacing of the defect with a pedicled split hypogastric flap. The cutaneous component was used for the volar defect, while the adipofascial component covered the exposed bony structures at the radial end of the dorsum of the hand (Figure 5A–D).
_volar_surface_of_the_left_hand__wrist__and_distal_forearm_showing_extensive_soft_tissu.jpeg)
_cutaneous_flap_component_in_situ_on_the_volar_defect__(b)_the_adipofascial_flap_compon.jpeg)
The design of the hypogastric flap and its splitting into 2 components are shown in Figure 6A and B. The pedicled flap was divided on postoperative day 14, and the granulated adipofascial component was covered with a split-thickness skin graft. Graft take and donor site healing occurred uneventfully. The radial fracture was also fixed with an implant by the orthopedic surgeon. Gentle active and passive physiotherapy continued postoperatively. A 3-month postoperative photograph showed stable wound coverage (Figure 5C and D). He was referred for prosthetic rehabilitation of the left hand but was last seen in the surgical outpatient clinic 3 months after the surgical procedure.
_design_of_the_hypogastric_flap_on_the_lower_abdomen__and_(b)_splitting_of_the_hypogast.jpeg)
Discussion
The introduction of the pedicled split hypogastric flap simplifies the otherwise demanding surgical resurfacing of complex hand defects in low-resource centres in sub-Saharan Africa, which generally face poor clinical outcomes in hand injury management.10 The rich blood supply of the lower abdominal wall, the distribution of the axial supply of the flap, the superficial inferior epigastric artery into the subcutaneous and subdermal plexuses, and experience with primary thinning of the hypogastric flap by removing loose adipose tissue deep to Scarpa fascia inspires confidence in the viability of the pedicled split hypogastric flap.9
Our experience of the survival of the 2 components of the split flap has further substantiated this innovative modification, extensively described by Sabapathy et al.9 The cutaneous component supplied by the subdermal plexus was used to cover the larger dorsal defect in the first case, while the adipofascial component reliably sealed the cavitary defect within the palm. With this, we achieved color match and prevented adduction contraction within the palm with a single flap. In the second case, a contiguous dorsopalmar defect was easily covered with the split hypogastric flap. The palmar defect striding the wrist joint received the cutaneous component, while the dorsal exposed bony structures were resurfaced with the adipofascial split flap that was secondarily skin grafted. This facilitated early rehabilitation, as the wrist joint and the gliding structures passing through the wrist area received supple tissue coverage.11
In both cases described, split-skin grafting of the adipofascial flap was performed at the time of pedicle division. Although primary skin grafting was reported by Sabapathy et al,9 we favored grafting at the time of pedicle division to improve the chances of complete graft take. Interestingly, both cases had flap division at 3 and 2 weeks, respectively, without any significant untoward events. Our unit policy is to divide pedicled flaps at 2–3 weeks, with optimal considerations of patient and surgical factors, while noting that axial vessel supply attrition has already commenced and that most flaps can then rely on the recipient-site supply. Moreover, this also reduces the duration of patients’ discomfort engendered by the hand-groin synechiae.12
The flap tip necrosis observed in the first case may be attributable to the stretch of the cutaneous component, resulting in microvascular spasm of the distal 2-cm segment. The necrotic tissue was debrided at the bedside and managed with local wound care; no secondary surgical procedure was performed. Measures were taken to avoid this complication in the second case, which healed uneventfully. Neither patient underwent tendon reconstruction, as this was not feasible primarily, and both patients were subsequently lost to follow-up. A recent systematic review and meta-analysis comparing pedicled and free flaps for hand reconstruction concluded that although pedicled flaps are associated with lower complication rates, they have higher revision rates than free flaps.13 Therefore, free flaps may remain the preferred option for achieving superior aesthetic outcomes in the reconstruction of complex hand defects.
The 2 cases presented illustrate high-energy-impact hand injuries resulting from handling hazardous objects (Table 1 Supplementary Material). The increasing occurrence of blast injuries to the hand in sub-Saharan Africa from mishandling of local Dane guns has been previously reported.14 However, a destructive hand injury from the explosion of a nitrous oxide cylinder has not been widely reported in our setting. Nitrous oxide, commonly referred to as laughing gas, is often used to inflate balloons at parties to produce a euphoric effect. Several complications associated with recreational use of nitrous oxide have been reported, particularly frostbite and myeloneuropathy, with attendant unwarranted morbidities.15–17 Of particular concern is the potential for massive damage to the upper limb caused by the high internal pressure of nitrous oxide cylinders. In the present cases, the pedicled split hypogastric flap provided durable coverage of the resultant defects and facilitated early physical, psychological, and social rehabilitation. We acknowledge several limitations of this study, including the small sample size, lack of objective functional assessment, and limited duration of follow-up, which should be addressed in future studies.
Conclusion
In this case report, we present 2 illustrative, challenging cases of the use of a pedicled split hypogastric flap. We believe that its simple design, ease of execution, and reduced operating time make it a promising alternative for selected cases in resource-constrained facilities in sub-Saharan Africa.
Acknowledgements
The authors acknowledge the patients’ cooperation in drafting this manuscript, as well as the use of the Grammarly AI tool to improve the text’s readability.
Ethical Approval
Institutional ethical approval was obtained from the Human Research and Ethics Committee of the Federal Teaching Hospital, Ido-Ekiti, with approval number ERC/2026/02/24/1493A
Informed Consent
Written, informed consent was obtained from both patients for the publication of the clinical details and accompanying images.
Data Availability
All the data supporting the findings of this case report are entirely contained within the body of the manuscript and its accompanying figures.
Conflict of Interest
None
Funding
None